
Thank you, readers, for a lively dialog that has developed at the bottom of this page over the last few weeks, touching on some subjects that I have written about and many that I haven’t written about. I will take this space to respond to some of what you’ve written about. Some of my favorite topics include exercise, epigenetics, NSAIDs, and the gut microbiome. Reports of whole-body rejuvenation with the four “Yakanaka factors” is especially promising. I’m grateful to Dr Paul Rivas for many of the ideas that I’ve expanded on here.
Aspirin, Ibuprofen, Naproxen
Background: COX2 inhibitors were found to reduce pain and inflammation of arthritis, but most COX2 inhibitors also inhibit COX1. It is the COX1 inhibition that led to stomach damage and ulcer risk. So in the 1990s, the pharma industry set out to find drugs that would inhibit COX2 without inhibiting COX1. Only later, it came to light that these drugs elevated risk of heart disease, though they lowered the risk of cancer. (Merck knew of the dangers of Vioxx before anyone else, but kept the stats under their hat as long as they could.) The worst offender, Vioxx=rofecoxib was taken off the market. Only after CV statistics made the problem clear, researchers were led to ask, Why? The problem is endemic. Turns out that COX2 plays a role in maintenance of arterial health, and generally the NSAIDs increase heart risk to the extent that they inhibit COX2. It turned out that Vioxx was dangerous because it did too well exactly what it was designed to do.
This story hangs together until we consider aspirin. Aspirin inhibits both COX1 and COX2, and yet the preponderance of studies appear to show aspirin is associated with reduced CV risk [ref, ref]. This suggests there is a piece of the metabolic puzzle that is still missing. Aspirin has many mechanisms of action, some of them unique to aspirin.
My advice, longstanding, has been to take ¼ to 1 whole aspirin or ibuprofen a day (not both; not to be mixed in the same week) after about age 50 for lowered inflammation and protection from heart disease and cancer. Evidence for protective effect of aspirin has weakened a bit in recent years, but is still holding up [2016]. For patients who have already had a heart attack, aspirin remains standard protocol, and evidence for this population is strongest.
Readers pointed to this study [2017], which reports elevated risk of heart attack for people taking ibuprofen or naproxen. The dosages they are looking at are several times higher than the daily dosage used for prevention alone.
All the NSAIDs have powerful effects in reducing cancer risk. Glossing over the different numbers for different kinds of cancer with different NSAIDs in different studies, it’s a good rule of thumb that taking low-dose NSAIDs daily cuts cancer risk in half. [ref]
Effects on cardiovascular risk are more complicated. I have been unable to find direct comparisons of aspirin vs ibuprofen and others, but there is “circumstantial” evidence in the literature that aspirin slightly decreases CV risk, while all the others slightly increase risk. Different studies rank the NSAIDs differently. There is suspicion of the “coxib” drugs which many people find work well for arthritis, but the latest studies show this seems to be unfounded. This study [2016] finds Celecoxib (Celebrex) is safer than either ibuprofen or naproxen (Alleve), and results in both lower CV risk and lower all-cause mortality.
There may be other reasons to prefer one or another NSAID. There are benefits for joint pain and stiffness; there are risks for gastric pain and ulcers. It’s an individual choice, and I encourage you to experiment on yourself. You can alternate different NSAIDs, but it’s best to do so week-by-week or month-by-month, rather than daily. Don’t take aspirin and other NSAIDs in the same week.
Does too much exercise cause areterial calcification?
Readers pointed to this study [2017] from Mayo Clinic, in which young adults were followed for 25 years, and those who exercised most hours per week had elevated calcification of their arteries. Calcification, in turn, is correlated with higher risk of heart disease.
There are several reasons I’m not turning on a dime to change my advice about exercise (which has always been, “the more, the better”).
- It’s a new finding. The study is still in preprint form, and cites no precedent.
- It’s based on just 268 subjects.
- The people in the high-exercise/high-calcification group did the equivalent of 7 or more hours of jogging each week. But the study didn’t separate recreational from occupational exercise. Social class is a really big factor, and it may be that all we’re seeing is that working class people have more CV symptoms than the upper middle class.
- The fact that exercise is correlated with calcification and calcification is correlated with increased heart risk does not necessarily imply that exercise is correlated with heart risk. This is such a common mistake. (A correlated with B) and (B correlated with C) does not let you conclude that A is correlated with C. In fact, the paper explicitly cites precedent that people who exercise most have lowest CV risk [ref, ref].
- So many benefits of exercise for so many aspects of health have been documented over the years that exercise is one of the solidest pillars of any health and longevity program.
The Copenhagen City Heart Study gave me more pause. They found that joggers who ran at a moderate pace 2-3 hours per week had longest lifespans. The benefit was about 6 years of life (a big number compared to every other life extension strategy that’s been studied, with the exception of caloric restriction). But runners who worked longer and harder than this lost the benefit and, in fact, died early. There is support for this thesis in other articles as well [ref, ref]. But there are also studies claiming that there is only a law of diminishing returns, and no amount or intensity of exercise that is actually bad for longevity [ref, ref].
I have not figured out the reason that different studies come to different conclusions, but here is what they agree on:
- Exercise has a strong benefit for life expectancy, health, mood and productivity.
- For low intensity exercise (yoga, walking, hiking, low-speed cycling, low-speed swimming) there is no evidence that too much can hurt you.
- If there is a threshold above which exercise can increase cardiovascular risk and shorten life expectancy, it is only for intense exercise and long duration, typical of a marathon runner.
My guess (based on disagreement among experts) is that there are individuals for whom a great deal of high intensity exercise is beneficial, and there are others who damage their cardiovascular systems by pushing too far. Doctors may be able to tell you if you have a heart condition that makes exercise hazardous. My hope (based on personal experience with yoga) is that we might develop a sensitivity to our bodies, so that we can distinguish the pain of damage from the pain and resistance that always accompanies a strenuous workout.
IP6 is a new supplement for me
I’m grateful to Dr Paul Rivas whose comment in this blog led me to read a little about it. Inositol hexaphosphate (IP6) is a bio-available form of Inositol, which is in the B-vitamin family. It has a major benefit for certain kinds of anxiety and depression, and minor benefits for blood sugar, insulin sensitivity, and cancer prevention.
Extraordinary story of radiation hormesis
A reader referred us to this story in a comment last week.
It would be unethical to intentionally expose people, unknowing, to ionizing radiation. But in Taiwan 35 years ago, construction steel was accidentally contaminated with Cobalt 60. The Health Safety Society recommends that 50 millisieverts (mSv) is the maximum safe radiation dosage. But 1700 people in apartments buildings in Taibei were exposed to this much radiation year after year for a period of 9-20 years until the contamination was discovered and they were evacuated. These people were studied for adverse possible health effects, but the result was that they had dramatically lower rates of cancer and birth defects.
Hormesis is a word for Improved health and longevity in response to challenges such as low doses of toxins, radiation, heat, cold exercise and fasting.
Cancer as atavism
Dr Green has outlined a theory that cancer [his comment] is a state of unconstrained cell growth characteristic of free-living cells half a billion years ago, before there was multicellular life.
First part of theory is cancer is normal growth from prior to 500,000 million years ago, prior to Cambian period. That was before plants and before oxygen rich atmosphere; life was fermentation, unlimited telomerase, no aging, cells were immortal.
This was new to me. Cyanobacteria have been around for 2.5 billion years, with the capacity to turn CO2 into O2. But apparently it was not until 800-600 million years ago that the oxygen in the atmosphere approached present levels.
Of more practical interest is Dr Green’s idea that it is epigenetics and not genetics that makes a cancer cell. If this is true, then an entire anti-cancer industry based on the idea of mutations being the root cause of cancer is misguided.
Yamanaka Factors Used for Rejuvenation
I missed this article when it came out almost a year ago. The “Yamanaka factors” (abbreviated OSKM) are four chemicals which, when applied together, can turn an ordinary differentiated cell (a skin cell, for example) back into the stem cell from which it came. Pluripotent stem cells replenish all the cell needs in the body. The offspring of a stem cell can be any kind of cell, hence “pluripotent”. Up until ten years ago, it was thought that this was a one-way street, and that the process of differentiation was irreversible. Then the Kyoto laboratory of Shinya Yamanaka reported success in “de-differentiating” cells by adding just four chemicals, initials O, S, K and M. In other words, these four chemicals turn a regular skin or muscle or organ cell back into the stem cell from whence it came.
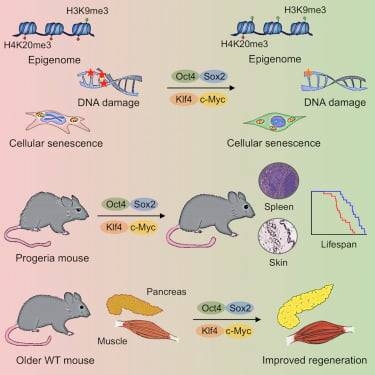
De-differentiation rejuvenates the cell, including lengthening of telomeres. But can the rejuvenation be done without the de-differentiation? That’s the subject of a Cell paper by Ocampo et al. They report success in rejuvenating cells in a living mouse, without changing them back into stem cells. They do this via intermittent doses of the same four Yamanaka factors. The shorter duration (2-4 days) has the effect of epigenetically reprogramming cells to their younger state, without destroying their differentiated identity.
For several years, I have have been attracted to the idea that aging is essentially an evolved epigenetic program. The holy grail would be to take cells that are programmed to be old and epigenetically reprogram them to be young. The hitch in this plan is that to do this directly requires changing methylation at millions of separate sites, in addition to re-programming dozens of other kinds of epigenetic markers (besides methylation), some of which are just being discovered. These sites are specific to cell type, introducing further complexity. We have neither the knowledge of where all these sites are, and only rudimenteray ability to alter them with CRISPR and allied techniques.
These results raise the exciting possibility that epigenetic changes supersede/precede other aging hallmarks in the physiological aging process, as well, and may thus constitute a key target for future rejuvenation strategies. – Anne Brunet & Salah Mahmoudi
The finding last year by Ocampo et al offers the possibility that we don’t have to do any of this, that just four chemicals will instruct the body to do it all for us. Watch closely—this may be the pathway to whole-body rejuvenation that so many researchers have been groping toward.
What about damage to the cells? The good news is that epigenetically rejuvenated cells seem to be able to repair their damage better than we might do it with artificial interventions. Somatic DNA mutations were repaired. Mitochondria were returned to a younger appearance and performance.
Provisos and qualifications:
- Lifespan increase has been demonstrated in genetically short-lived mice. For normal lab mice, they report physiological markers of rejuvenation, but didn’t wait to see if the mice would live longer.
- How do you get OSKM into the mice (or the humans)? In this experiment, extra copies of the four factors were inserted into the mouse genome before birth in such a way that they were normally turned off, except in the presence of the antibiotic doxycycline. This provided a convenient way to turn OSKM on and off at will, with injections of doxycycline.
- In the genetically short-lived mice, the rejuvenation is temporary, only lasting 8 days before progeria asserts itself again. We don’t yet know whether rejuvenation in normal mice will be short- or long-acting.
Brunet and Mahmoudi end by suggesting that induction of the four factors could be combined with removal of senescent cells, speculating that major life extension could result from synergy between the two. (They also note that getting the four factors into cells of a living human being is a challenge we don’t yet know how to approach.)

News from the world of telomerase activation
Thanks again to Dr Rivas for this article demonstrating that ashwagandha is a potent telomerase activator. This article adds to the evidence that cells with the shortest telomeres are the problem, and average telomere length is less important.
Gut Microbiome
Once again it is Dr Rivas pointing us to this article. Stool samples from 1,000 “extremely healthy” people of all ages were analyzed for RNA sequences associated with intestinal bacteria. Their principal finding was that the composition of the bacteria depended more on health than on age. There were major differences through childhood, and for people in their 20s, the bacterial colony was in a class by itself. But after age 30, up through age 100, bacterial ecology of all the healthy individuals tended to look alike.
A recent consensus says that we lose gut diversity with age, possibly as an adaptation, but more likely with negative consequences for health.
Tocotrienols
These are variants of vitamin E. They differ from vitamin E (tocopherol) in the same way that unsaturated fats differ from saturated fats. They are more reactive, more easily manipulated by the body. The normal varieyty of vitamin E (alpha tocopherol) does not have lifespan benefits, and may be a net negative. Gamma tocopherol may be better, or it may be that we need a mixture of tocopherols in combination. The only human studies have been done with alpha tocopherol, and when you buy “vitamin E pills” that’s what you’re getting.
Early research suggests that tocotrienols protect against cancer and reduce inflammation. The body treats them differently from vitamin E, and they have separate activity. Tocotrienols occur naturally in foods including palm oil, wheat germ, and rice bran. You can buy supplements of mixed tocotrienols, or gamma tocotrienol, or mixed tocotrienols with tocopherols.
Inheriting Telomere Length
Unsurprisingly, telomere length at birth is inherited from parents, and is assumed to be correlated to lifespan. Surpringly, a baby’s telomere length is inherited more from the father than from the mother. More surprisingly, older fathers sire children with longer telomeres (though their own telomeres are, presumably, shorter).
Low-Dose Naltrexone
Naltrexone is a 35-year-old drug used to block opioid receptors and help people breaking addictions. Soon afterward, Dr Bernard Birhari discovered naltrexone in low doses as a treatment for auto-immune disorders (allergies, lupus) and as an anti-inflammatory. There has been some success with LDN as a cancer treatment. Take LDN at bedtime, as it blocks pleasure receptors. The theory is that blocking receptors during sleep increases the release of endorphins during the day. There is anecdotal evidence for LDN as treatment for depression, PTSD, anxiety and sexual dysfunction. LDN hasn’t been approved or tested for any of these uses, but informal experimentation off-label is gathering a critical mass. Advocacy site for LDN.
Thanks to all of you reading this column, and thanks especially for the intelligent and informative conversation that has grown up underneath this blog. I hope you’ll please keep the ideas coming!
Discover more from Josh Mitteldorf
Subscribe to get the latest posts sent to your email.
Josh,
why did you write that you missed the OSKM rejuvenation paper?
You reported it in december 2016
https://joshmitteldorf.scienceblog.com/2016/12/23/from-santa-diego-a-jolla-xmas-gift/
He meant he missed the review paper by Brunet et al.
Josh, did you know that a company called Youthereum Genetics is being set up in Russia with the aim of doing epigenetic rejuvenation in humans?
It seems to be a credible effort. The founder was interviewed recently at Fight Aging.
Oops, my comment that Josh is one of our scientific advisors seems to have been posted outside of this thread. Please see below.
Whoops! You are obviously are well aware of this then, Josh!
My thoughts on excessive high intensive exercise is that it may be the depletion of essential minerals (such as magnesium), may lead to worse health outcomes. This may be because it would then lead to poor blood sugar control.
I say this because as a heavy gym user (combined with excessive alcohol use), I suffered muscle twitching and some high blood sugar episodes (resolved by giving up alcohol for a week and going low carb).
I think for those from colder climates excessive sweating should also be avoided for this reason. For those originating from hotter climates I believe the converse may be true – I think they should be sweating to help out their kidneys excrete and/or keep their proteins level low – the UK’s population from the India sub-continent suffers kidney failure at a significantly higher rate than the indigenous population, even when both have type 2 diabetes.
I actually think the beneficial effect of alcohol health wise ( which is generally put at not more than a unit or two a day – which would normally be taken with a meal), may also be the result of it delaying the release of sugars into the bloodstream.
Josh
Excellent, detailed and comprehensive as usual.
One of your readers( Ea) made me aware of a study on tocotrienols in relation to cellular senescence. Incredibly this study shows a promotion of senescence in cancer cells, while preventing senescence in normal cells, and also acting with quercetin as senolytics to clear already formed senescent cells.
eurekaselect.com 134723. Pleiotropic Effects of Tocotrienols and Quercetin on cellular Senescence.
On ASA and NSAIDS. Maybe as you say one week ASA and next week celebrex.
Regarding exercise and calcification, I read the paper when it was mentioned 2 weeks ago, and there were many things not measured. Those doing the most running are fueling themselves how? Probably carb loading etc, but nobody is measuring insulin, especially Kraft insulin assays. The person most responsible for publicizing Kraft’s work in recent times is Irishman Ivor Cummins. He’s “only an engineer” (albeit with a biochem and problem-solving background) but more and more MDs are paying attention to him. Measures of hyperinsulinemia are much better predictors of CVD than cholesterol etc. (Also, CAC scores are king as Paul Rivas mentioned.)
http://www.thefatemperor.com/blog/2015/5/10/lchf-the-genius-of-dr-joseph-r-kraft-exposing-the-true-extent-of-diabetes
Thanks for the mention, Mark. Josh is actually one of our scientific advisors (all our SAB and team members are listed on our website at http://www.youthereum.io). For me personally, Josh has had a great deal of influence on my understanding of aging and on how epigenetics can be one of its key implementation mechanisms.
I like your website a lot Yuri.
I’ve read a couple of a papers that suggest you can improve on OSKM quite considerably by including some extra factors. According to this paper: ‘Two Supporting Factors Greatly Improve the Efficiency of Human iPSC Generation’, you can improve the efficiency of reprogramming by 100 times using either p53 siRNA or UTF1. Now I know you don’t want to go all the way back to pluripotency, but this might still be useful.
Also: ‘Rejuvenating senescent and centenarian human cells by reprogramming through the pluripotent state’ showed that adding NANOG and LIN28 allowed the rescue of senescent cells.
Thanks, Mark!
Another promising indication that cyclic OSKM induction can reduce or prevent senescent cell burden is the fact that beta-gal levels were greatly reduced in livers of treated mice in the Ocampo/Belmonte paper.
Hi Yuri,
your company looks really aspiring. I wish good luck to you and your team.
As cost reduction might be a key point for you, have you thought about using C: elegans as a model organism?
Ihavent yet seen a paper with IPSC generation of C.elegans, though I believe it should be doable.
This is a risk since no one is doing it, but also an opportunity to have a much faster feedback cycle than mice.
And should be much cheaper.
At least this article suggests that the epigentic drivers of aging are present in C. elegans and Drosophila, too.
http://advances.sciencemag.org/content/2/7/e1600584.full?utm_source=sciencemagazine&utm_medium=facebook-text&utm_campaign=epigenetics-6189
Hi Josh,
Very nice summary of epigenetic cancer theory. Weinberg first presented that theory @ 1983 and showed demethylation of cancer cells. Major theory is cancer due to new mutations genes and minor theory due to epigenetic changes due to demethylation.
Plants started @ 500 million years ago and began changing atmosphere from CO2 rich to more oxygen.
Idea that original life resembled cancer from astrophysicist, (don’t remember name) but you mentioned you were big fan of his.
Intuitively, hard to understand how cancer could be so metabolically robust if had to rely on de novo mutations. On the other hand, if cancer was a life form that had evolved over a billion years; then makes sense that cancer is such a robust life form. The other intuitive problem with mutation theory is as cancer becomes more undifferentiated, they all look the same. One would think if each cancer was it’s own set of new and different random mutations, cancers would all look very unique. As regards poorly differentiated cancer, microscopically, you’ve seen one cancer, you’ve seen them all.
As regards continuing need for oxygen free growth; human fetus needs that ability in first week of life, until implantation in uterus and finally gets an oxygen rich blood supply. A four day old fetus looks a lot more like cancer than adult tissue.
It might be that both epigenetic and genetic changes are occurring. I agree that it is most likely an epigenetic change that activates a pre-existing ‘oncogene’ or as you put it a primitive life growth gene. But cancer then has to go through a crisis when it forces the cell to go past replicative senescence and override p21 arrest. This uses up the last remaining telomere and the generates a DNA double break. Most cells die at this point. But a very, very small minority manage to continue. This is the point at which an actual genetic mutation has occurred IMO. So in my view an epigenetic change is then leading to a real mutation. If this is true then prevention of cancer should focus on epigenetics, but cure may require genetic treatment.
Paul Davies.
This guy rips into him. Opinions please? ; – )
http://scienceblogs.com/insolence/2017/07/18/a-physicist-clueless-about-cancer-
lectures-cancer-biologists-on-cancer/
(Ok, looks like I have to write more to get around the spam filter.)
Cheers,
Nick.
On combining epigenetic reprogramming and senolytics, this paper would suggest this might be unnecessary: ‘Rejuvenating senescent and centenarian human cells by reprogramming through the pluripotent state’, PMC3219229.
They used six factors, not four: OCT4, SOX2, KLF4, and c-MYC (OSKM) plus NANOG and LIN28.
Incidentally this was the paper that convinced me (not the work on progeria mice Josh has posted about previously) that epigenetic reprogramming might actually work in humans.
Thanks for all your research Josh, I read what I can and am from a non scientific background.
I am from Ireland and waiting on a hip replacement and since May this year have beentaking 250 mg of naproxen twice a day.
I am 56 yr old female on no other medication at all. I have always had an inclination to bleed a lot from small wounds and cuts.
If you were me would you alternate painkilling medication , and if so with what. I think I will be waiting about another 12 months for op and need pain killers each day.
I also swim 20 mins every other day in the sea throughout the year, as you can imagine Ireland is rather cold and this morning the water temperature was about 12 degrees. Have you any views on cold submersion?
Swimming is the only exercise I can do, and I hate heated pools.
Interested in your views.
Aspirin has a number of other mechanisms than COX inhibition (as you pointed out Josh), one of which is that people who take it for a long period of time have lower iron levels, some 25% or more lower. This happens because aspirin promotes minor intestinal bleeding, and possibly also because aspirin directly chelates iron. (The chemical assay for salicylates involves adding ferric chloride to a solution, which binds to salicylate and turns blue.) Iron lowering could account for much of aspirin’s anti-cancer activity and some of it’s long-term CVD prevention. Salicylate is among the most powerful iron chelators and is in fact used by some species of bacteria to grab iron from their host.
Willow bark extract was found by Titorenko and colleagues to be the most powerful life-extension substance on yeast yet found, and of course willow bark contains salicylate.
PD Mangan you have fantastic site Rogue H & F I have been referring to many times in the past. Aren’t there other ways to chelate excess iron to prevent cancer without the side effects associated with salicylates? Also can there be some other cause also for the life extension shown by Willow Bark?
Thanks Akshay, yes indeed there are other ways to get rid of iron and/or chelate it. I’m just pointing out one of aspirin’s likely other mechanisms. Yes also that willow bark could and probably does have other components that are important. Some research concluded that the salicylate in willow couldn’t possibly account for all of its painkilling ability since there’s too little compared to aspirin.
I also have to say what a great site this is. Josh continually writes the most interesting stuff, and the commenters here do so as well.
Does anybody here know who is xEva forum member at Longevity? We independently came to the same conclusion on mechanism of aging so am keen to swap notes.
Hi P.D.
I read your book, Dumping Iron, and have to say that many of your thoughts there make a great deal of sense. The idea that many of the beneficial effects of ASA could be due to slow blood loss and the resultant decrease in ferritin levels is both clever and original. It fits with even the latest evidence that ASA takes 5 years or more to give protection. It also makes sense in pre-menopausal women who have low ferritin and low heart disease, but this protection disappears in menopausal women who no longer bleed. Estrogen clearly wasn’t the answer.
Well done
Hi Paul,
This study is the most serious I have found about ferritin and mortality:
“Total and Cause-Specific Mortality by Moderately and Markedly Increased Ferritin Concentrations: General Population Study and Metaanalysis”
There is a clear association between ferritin level above 200 and higher mortality. However, anything below 200 seems to be fine. Do you have some evidence that ferritin should be lowered even below 200?
Joanna Russel Professor of evolutionary biology University of Arizona has outlined their findings which is recently published in the Proceedings of the National Academy of Sciences that they claim ‘proves’ aging is mathematically inevitable – like, seriously inevitable. There’s logically, theoretically, mathematically no way out. Their study is called Intercellular competition and inevitability of multicellular aging. Pretty depressing if it’s irrefutable.
Remember we don’t need to create an immortal body that can perpetually remain in homeostasis (between senescence and cancer). If this paper goes unrefuted, then this is impossible anyway.
We only need periodic treatments that can reset homeostasis to a more youthful level. Senolytics, lengthening telomeres and epigenetic programming all promise to do just that.
And while we are waiting there is nothing in this paper to suggest we cannot do considerably better than the current human lifespan.
I agree with Mark,
This paper does not refute that human life span can be considerably extended from what it is currently. We could have an average life span of 1000 years without violating any of its hypothesis.
Secondly, one of their assumptions is that somatic degradation does happen inevitably. Note that this is not a proof but an assumption. You could argue that in the 23th. century, we’ll have the technology (think nanotechnology, nanobots, ..) to prevent that. At that time, we will be in total control of our genome stability. Just a speculation.
“First, we assume that somatic degradation is nonzero. Kogan et al. (46) point out that gene networks can be indefinitely stable if cellular repair mechanisms are sufficiently effective, raising the possibility that cellular degradation may occur at a rate of zero were selection on repair mechanisms somehow made sufficiently strong. However, as the ability to avoid or repair cellular damage is itself a trait subject to degradation, the rate of degradation will likely increase with age as the genetic factors that constrain errors are themselves degraded (47, 48). Thus, the rate of cellular degradation may accelerate through time, precluding indefinite stability”.
Mark Aldebaran well concluded. By the way Mark this is one of the key focus of my Lab, if you remember, to upreguate the degraded repair systems back to maintain homeostasis so in a way I am glad I am attacking the very backbone of their theorem that inversely leads to inevitable loss of life but the damage and repair interplay at this time juncture seems so alarmingly complex. But 8 too am an optimist and agree with both of you that we humans have the capacity to find the technology sometime in the future.
Hi Akshay
I think it’s likely that before we get to the high tech stage suggested so aptly by Aldebaran, some if not most of the answers in the near future at least , will involve medications like rapamycin, rifampin, cardiac glycosides, beta blockers , ACE inhibitors, etc. Which brings me to this story.
Recently I had to go see my idiot doctor( ID) to get an insurance referral for an echocardiogram that I want to check my cardiac ejection fraction. I’m positive that it’s gone up since rapamycin 3 months ago because of the way that I can now take hills.
So he looked at my huge list of supplements and rapamycin ( which he had never heard of). So ID says to me:
1. You know all of these “vitamins” that you take have been “proven” to do more harm than good.
2. Look at you, you’d better stay out of the sun, you’ll get skin cancer ( ignoring my vit D level of 60, and that 90% of skin cancers are benign c/w most cancers associated with low D that will actually KILL YOU).
3. What’s this rapamucin stuff you’re on? You know you shouldn’t take antibiotics for too long.
4. Why do you want an echo? Did you have a heart attack?
5.Where’s your PSA level? After all, it’s all we’ve got.
( So better to get a test that doesn’t effect mortality rates because “it’s all we’ve got”.
Now I point all of this out in empathy with most of you who aren’t in this profession and have limited options regarding your medical care. It’s a fact that most doctors will be unwilling to treat aging as some sort of illness. Not now. Not ever. So no matter what discoveries we make, if it involves meds , it’s going to be difficult.
Now to be fair, there are some excellent and open minded doctors out there, but I find that they tend more to be subspecialists with a high degree of training. Like my friend and associate Daniel, trained at Harvard in internal medicine, will not just dismiss you, very open minded.
As an aside, I saw a guy the other week, the husband of a patient, who told me that he had terminal lung cancer. He went on to say that he goes to an oncologist from Russia who gives him weekly Mistletoe injections.
I told him that I had never heard of that.
He said ” well my tumors are 90% gone now”. “What do you think I should do?”
I said I don’t really know, but if I were you I’d double down on the mistletoe!
And while you’re at it, Save some for me.
Mistletoe injections must research that! Paul we know which category you fall under as a doctor. Very highly informed and open minded.
Speaking of idiot doctors…It would be enormously helpful if people here who have doctors who are knowledgeable – or at least open – to recent aging research would consider sharing their names. My own doctor, thought not an idiot, has severe limitations (she told me that fasting more than 16 hours was dangerous and refused to look at an article about Longo). Doctors who proclaim to be anti-aging often have cheesy websites. It’s hard to find a good doctor without a trustworthy referral.
Thank you, Josh, for your extraordinary site and everyone here who contributes. I’m a determined to stay healthy 65, and this site has given me enormous optimism about aging pro-actively. I am not a scientist, so a lot goes over my head, but the discussions fascinates me. Besides being beneficial for my heath, Josh’s site has made a new world of biological research accessible to me. I so appreciate having a ringside seat!
Lindy it’s post like yours that encourages Josh and community here to share information here. I would recommend Dr. Paul Rivas and Dr. Alan Green
Hi Lindy,
A few words in defense of my fellow physicians: Doctors follow what is in medical textbooks. Medical textbooks don’t recognize aging as disease and have zero discussion of aging. As far as medicine is concerned, aging is natural condition; end of story.
Also almost all doctors believe in human clinical trials for translation of basic science into office practice. Rapamycin is generic drug so nobody spending hundreds of millions of dollars on clinical trials.
Also doctors are busy. They read journals in their specialty. They don’t read basic science stuff.
So very hard for physician to discover Blagosklonny. Realize Blagosklonny is greatest scientist since Charles Darwin and then become expert on Rapamycin. Also no medical literature explaining how to use Rapamycin as anti aging drug.
Also getting old and getting sick is a trillion dollar industry. What would happen if old people refused to get sick.
Hi Paul,
Excellent post.
Really funny and right to the point.
The number of times that I am told I don’t need those ‘vitamins’! Great story Paul.
So rather than kissing my wife under the mistletoe this year, I’m going to reach up and eat the stuff, thus confirming what she’s always suspected about me.
Great job Akshay, you are definitely on the right track in my opinion. Please keep us informed how your work is going.
This paper reminds me of the story I was told at University about the difference between an applied and a theoretical mathematician. They stood in opposite corners of a square room and in one of the other corners between them, stood the most beautiful women either of them had ever seen. They were told, whomever can reach her, can have his way with her. But to reach her you must take each step half the length of the step before it. The theoretician realised there was no point even trying, as she was some way from him and with each step he would only make up half the distance of the step before it, so could never actually reach the girl. But the other man just gave it a try, and soon realised that although he could never get to zero distance from the girl, he could get close enough!
Anyway the point is, small efforts will add up, and decades more of healthy life are probably not all that far away.
Thanks. good story on the mathematicians 🙂
Hi Paul:
The mistletoe extract is known as Iscador. USA physicians are allowed to order and administer Iscador under “compassionate care act” rules.
There was an actress named Suzanne (sp) Sommers, who had breast cancer about 12 years ago and opted to use Iscador injections.
She is still alive, and wrote at least one book outlining her experience.
Paul:
To Add to Iscador post, the extract of Mistletoe is used because the leaves and berries of mistletoe are reportedly poisonous.
Just sayin’… I think you were likely joking about eating the Misteltoe plant.
Hi Heather
Interesting post about Iscador. I had never heard of it . You wouldn’t believe the things I hear at least once a week. A guy with a crazy high prostate cancer PSA reading said that his level completely normalized using 1 gram of cbd oil a day from hemp. Who knows? There is a fascinating study showing multiple anti-cancer pathways of cannabidiol.
Cannabidiol as potential anti cancer drug
Paola Massi Br J Clin Pharma. 2013 Feb 75 (2). 303-312.
I really do believe that even now with the proper diet/exercise/supplement/medication regimen that we could realistically prevent 95% of the age related diseases.
Hi Paul:
Interesting information on the CBD oil and the anti-cancer Cannabidiol pathways.
Your patients are lucky to have an open minded doctor.
As Shakespeare wrote for Hamlet to opine:
“There are more things in heaven and Earth, Horatio, / Than are dreamt of in (y) our philosophy.”
Reading your post, thank you Aldebaran, something came as a flash to me: are they somehow assuming what they are supposed to “prove”? They assume that somatic degradation is non zero and then they prove that somatic degradation is non zero! I must have it wrong as it looks too simple and I must have it wrong when making somatic degradation equivalent to multicellular aging.
And yes I agree with you the paper says nothing on time frames (Josh makes the same point in his post, see below) and future technologies.
I hope for a published rebuttal of this paper, see also here:
https://joshmitteldorf.scienceblog.com/2017/11/09/aging-in-the-news-this-week/#comment-382737
Even if only one of the three basic assumptions is wrong:
– somatic degradation is nonzero…
– independence of multicellular vitality from developmental programming
– negative covariance between vigor and cooperation the
…the “proof” would fail.
Just in case you have overlooked it Josh and Greg Fahy have a published rebuttal in PNAS here: https://drive.google.com/open?id=1VcLlb0TXhlYZr38UQSgskOKm1Njva_68
Hi Josh:
You did a good job in pulling everything together succinctly, in one article.
I was also glad to find Paul Rivas suggestions regarding IP6 and the suggested proper ratio of the Inositol to Inositol hexaphosphate.
Correlation between telomerase and mTOR pathway in cancer stem cells.
https://www.ncbi.nlm.nih.gov/pubmed/29074462
Do we have any clue about mTOR decreasing telemorase in normal non cancer cells?
That is interesting and I’ll have to read the paper, but I think the key thing to remember is that TERT is like a growth hormone. So its expression will be correlated with MTOR. Think of high MTOR spurring proliferation of new cells and you get the point.
It is not suprising that Rapamycin and Telomerase activators are acting in opposite directions, as Rapamycin is basically the best calorie restriction mimetic we have, whereas telomerase stimulates growth.
I would suggest not combining the use of rapamycin and telomerase activators on the same day. But in general somatic cells express little or no telomerase, so MTOR inhibition is not going to harm them.
Jahahreeh Finley did a nice write up on Metformin, Methylene blue, rapamycin in regards to AMPK and its relevance for telomeres.
https://ampkprogeriahiv.wordpress.com/2017/01/08/metformin-and-exercise-shown-to-promote-telomere-transcription-and-integrity-via-ampk-activation-connection-between-progeria-aging-hiv-1-latency/
Very interesting, thanks for that – I was not aware of that blog, or of the connection between AMPK and telomeres via TERRA.
It’s certainly a complicated picture. Here we learn that MTOR inhibition (or AMPK activation) is actually preserving telomeres by unregulating the shelterin protein TERRA.
It hangs together nicely with the idea that being in an energy deficit state makes the body last longer.
Hi Mark,
Comment about TERRA and mTOR inhibition preserving telemeres very interesting. Clear from Ellizabeth Blackburn that lifestyle to preserve telemeres and lifestyle to lower mTOR huge overlap.
Also being energy deficit is beneficial as lowers mTOR pathway.
So Josh, as if right on cue with your post , this study of aspirin and cancer came out today from the Chinese University of Hong Kong, Kelvin Tsoi presented it at the United European Gastrenterology meeting in Barcelona.
They looked at 600,000 people over 10 years. Of these, 206,295 were ASA users. Average age 67.5 years, median dose 80mg and average duration 7.7 years. The team followed outcomes for up to 14 years looking for cancer incidences.
About 16% developed cancer, withlung being the most prevalent.
So here it is, the ASA users were:
47% less likely to have liver and esophageal cancer
38% less likely to have stomach cancer
34% less likely pancreatic cancer
24% less colon
Also significant reduction in leukemia, lung and prostate cancers
Wow
We knew it was good, but not this good!
Seems to have a ton of different mechanisms, which no one has unpicked yet.
Is White Willow bark more gentle on the stomach, and would it be worth starting before you are 50?
The salicin in White willow bark extracts is supposed to be gentler on the stomach than acetylsalicylic acid.
Also it contains additional ingredients other than the salicin that may have a synergistic effect and/or additional benefits.
For example a standardized product may contain Willow (bark) 500 mg
Willow (bark) Extract standardized to 15% salicin (60 mg) 400 mg
I have never seen an enteric coated white willow bark product, but it may be a good idea.
The good news is that the very low dose aspirin was effective. A low GI bleed risk at this dose, especially compared with the risk of cancer
An old psyche in a young body
Let’s suppose that someone discovers a rejuvenation mechanism and rejuvenate himself from 70 to 40 (not to say more). The psyche ( the total lifetime experiences) remains the same. Such a person would feel in the course of time very frustrated because of the discrepancy between the psyche and the body. Further when his psyche will be 100 years old will be very hard to keep pace with the 40-50 (as he body is). The brain as a neural network has a huge but limited capacity of adaptation.
I am very healthy and have a happy life but I don’t want to live over 70. Enough is enough.
See if you feel like that when you 69 and 364 days and get back to me 🙂
There is a joke: a man ask his doctor: „Doc, if I eat only healthy foods, have an active life, don’t drink, don’t smoke, etc. would I live 100 years. The doctor responds: I can’t guarantee that you will live 100 years, but I guarantee that you will feel it like 100 years
So you really don’t want to live over 70? That is crazy! Alan is over 70 and is fit and healthy. My own father is 77 and doing well. You are saying you want to live a shorter than average life expectancy. Now I would understand if you were to say living longer than 70 is conditional on you being in good health, but since you are here reading this blog, you must know that is a pretty good bet.
Many AI researchers assume that the brain is a neural network, but the brain does a lot of things that neural networks can’t do, and even one-celled protozoans can learn and respond in ways that show a primitive intelligence, though they have no nerves and no neural networks.
– JJM
I’ve often thought that one of the brain’s greatest abilities is the ability to forget. Hence I would be quite surprised a rejuvenated brain would have any difficulty adapting to existing in a rejuvenated body.
To rejuvenate the psyche is to forget. But in the long run, this would be the same as being totally another person. The death accomplished the same thing but abruptly. It can exist only a limited number of persons that rejuvenate and this way they become other persons. But in this case, the reproduction should disappear. Otherwise, the life wouldn’t be sustainable.
I see my own life just like an instance of LIFE. The other people and beings are other instances of life. When I die, only the instance that is represented by me dies. but LIFE goes on. I don’t want to rejuvenate and the instances to change ‘‘smoothly‘‘ and to carry some time ‘‘ the burden‘‘ of previous instances. Death solve this and allow the instances to start without any psychic connection with previous instances
And that is your choice, which I respect.
I hope to be able to make a different choice; the choice not to fall prey to the diseases of aging.
“To rejuvenate is to forget “. Not sure about that one. In order to carry on into the future the brain handles to a large degree both life extremes of extraordinarily good and bad . For instance, it has been shown that if you compare a lottery winner with a recent quadriplegic, the lottery winner is initially ecstatic while the accident victim is depressed, but one year later the brain has equalized the events so well that both groups report an almost identical degree of happiness and life satisfaction . Neither group has forgotten the past events, but both are indeed rejuvenated.
I’ve been filming scientists on aging research for 11 years, during which, its wide implications have gripped me. I homed in on something G B Shaw touched on in his play “back to Methuselah,” where in the Barnabas Brothers,
one an ex-clergyman, the other a biologist, posited “that the duration human life must be extended to 300 years; not because people would profit by a longer experience, but because it was not worth their time to make any serious attempt to better the world or their own condition, when they only had 30 or 40 years before they doddered away to decay and death.” according to Shaw, “its is our expectation of life and not our experience of it that determines our conduct and character. Consequently, the very vulgar notion that you cannot change human nature is valid only on the assumption that you cannot change the duration of human life. If you can change that, then you can change political conduct.” Thus spoke G B 100 years ago. I’ve devised a series incorporating this idea as a springboard to tackle the evolving psychological and political impacts. Indeed I see this new science as providing an end run around the status quo of the way we practice politics and business. I am hopeful.
There is some wisdom here in recognition that our lives are an instance of LIFE. Death in this context is enveloped by life which is a kind of inspiring an liberating idea. I still want rejuvenation and to go to 120 though because there are things I want to do/contribute to.
A brain is a network of neurons i.e. a neural network (a single neuron is also a network and so on). The immune system is also a network. In general, a system can be considered a network.A living organism is a network. When dies the network dissolves in smaller networks.
The maximal age for humans is about 125 years. And this remained constant despite medical progress. In the future with all the measures that you said and the ones that will come, more and more people will approach this limit, a few will survive a little bit beyond but that’s all. With all rejuvenation techniques, it will never pass past 200 years. This can be proved on other beings(considering their maximal age).
Humans are by far an incredibly unique species in the known universe. Which is why we should be cautious before any conclusive assumption that 200 years can never be crossed. At this vantage it may seem so but if an Egyptian scholar or an Indian Rishi 2,000 years ago said that one day humans will communicate across the world within seconds telepathically their peers must have surely mocked them but today we take this for granted. We have what is called in Sanskrit ‘Brahmastra’ the ultimate weapon: the ability to manipulate matter. This can create unthinkable opportunities. For example we can create nanobots powered by solar radiation mining nearby planets which can build millions of nanobots like bacterial multiplication which would then work from trillion different points to create another planet in our orbit based on a design mesh. This sounds absolutely crazy today but to me it’s absolutely possible. Our biology is a finite system and a finite system can be mastered one day. This is biggest incentive of a long life the wondrous amazement if seeing mind boggling technologies being revealed/discovered.
I agree Akshay, and had to hold myself back from making such ‘crazy’ statements in my previous comment, which I actually think are not at all far fetched.
For those that decide not to partake of rejuvenation technology, they should consider the future possibilities they will be missing out on.
As for the argument humans have an immutable maximum lifespan, I think that is very unlikely, given the advent of future technologies we cannot imagine now. Even now, with nothing but repurposed prescription drugs and supplements/life style interventions we are achieving a great deal. Soon genetic and epigenetic treatments will become commonplace, in fact intrepid types are already experimenting on themselves. This is just the start.
Do you really want to miss out on the 21st century?
This should be done first on very simple forms of life. For example, can be made a bacteria to live (and be functional !) 10 time more as the average lifetime for that bacteria? I mean for a particular individual bacteria in a colony not the average life of a colony to survive, because you refer to an individual.person.
Interesting discussion
Here is a link to an article discussing age reversal research.
https://www.scientificamerican.com/article/aging-is-reversible-at-least-in-human-cells-and-live-mice/
—————————–
From the article:
“By tweaking genes that turn adult cells back into embryoniclike ones, researchers at the Salk Institute for Biological Studies reversed the aging of mouse and human cells in vitro, extended the life of a mouse with an accelerated-aging condition and successfully promoted recovery from an injury in a middle-aged mouse, according to a study published Thursday in Cell.”
———————————————-
I think there will be many sociological pros and cons to living forever and in good health.
Even now. with short life spans. there is such a high rate of suicide among healthy people.
I do not think everyone wants to live forever.
Still, having the option is a good thing, IMO.
Florentin,
In the following paper, it is shown that a simple genetic manipulation can make worms live 10 times longer.
“Remarkable longevity and stress resistance of nematode PI3K-null mutants”
http://onlinelibrary.wiley.com/doi/10.1111/j.1474-9726.2007.00348.x/full
The discussion is not about whether or not the life could be prolonged. Certainly, it could. We are talking about whether the maximal life could be significantly prolonged.
For example for the House mouse, the maximal lifespan is 4 years. If there could be genetically manipulated (or otherwise) that a mouse could live more than 6 years then we could speak about the pushing up the limit
Natural processes are all irreversible processes. So the aging couldn’t be reversed it could only be slowed with all the consequences. For example, If the aging could be slowed 10 times then, the humans could live 1000 years but also the activity of the brain will be slowed accordingly so 10 years will be perceived (in average ) as 1 year.
What you say Florentin makes theoretical sense,but I’m not sure that it works that way. I’m on an mTOR inhibitor which is slowing down aging but I don’t believe that my brain activity has slowed as a consequence, in fact it feels sharper actually.
That mTOR inhibitor slows at best with few percents in average. One couldn’t possible sense this.
For example when after long fasting a man enters in starvation mode the metabolism decrease dramatically. In all situations when persons entered in starvation mode they sensed a contraction of subjective time. The last week of starvation seemed like 2-3 days.
In the case of old people, time flows faster subjectively compared when they were young
I must respectfully disagree Florentin. There is nothing about aging or CR which grants us the power to disrupt the space-time continuum. This is just perception at best, but perhaps not even that. This was actually studied by Wittman and Lehnhoff in 2005 where they looked at 499 subjects aged 14-94 and asked them questions about the passage of time . To their surprise there was not a significant association between age and the individuals’ perception of time. EVERYBODY , regardless of age, thought that time was passing quickly.
In 2010 Friedman and Janssen from Duke again looked at this with 50 students and 50 seniors to assess their perception of time. They found that people who experience time pressure, or not enough time to get everything done, are the ones where time passes quickest. Again, just a perception.
My experience with those who starve themselves for a week is that the last 3 days feel like 3 weeks!
Florentin:
Do you mean perceptually time will slow?
If so, I agree, that may be a possibility. 10 years my fly by as quickly as on in our minds.
Meant to say MAY fly by as quickly as one.
Sorry, but this is rubbish Floretin. We are not talking about slowing aging. Certainly that is what many current interventions do. But we are looking to epigenetic reprogramming, telomere lengthening, senescent cell removal, etc, which we have on the horizon now. These are all rejuvenating treatments because they are rewinding the clock or removing damage that has accumulated through the action of our metabolism over the years. These treatments will in some sense reverse aging and leave you in a younger state than your were before. You will likely continue to age from that point, but from a younger starting point, hence extending your life. This is well established by numerous papers, many of Josh’s blog posts, and our previous discussions. Your perception of time will not change, as your brain will be a young brain, so you woukd not have issues keeping up with change, as old people do now, although your perspective will be that of a person who has been alive longer than your appearance would suggest. This, I imagine will lead to a wiser, more humane world.
Ok, we could act against one of the fundamental laws of nature: all natural processes are irreversible.
Is this a fundamental natural law? Because for example Turiptosis a species part of nature ages and then reverses back to embryonic stage.
Hi Akshay,
Your commert about immortal jelly fish very interesting.
Thanks Alan
I quoted G B Shaw in a reply above, who posited that human nature is itself a function of lifespan. Take a look,
it implies wisdom is would be generated and political behavior altered.
Hi Robert:
Good points.
There is no law of physic that force natural processes to be irreversible as long as they can receive energy from outside. In practice, I agree that most biological processes might be very hard to reverse though.
I don’t think the brain of a naked mole rat is slower than the brain of a typical rat but the naked mole rat live for about 30 years while the typical rat live for 3 years.
As for mice living longer than 6 years. This is not far away. Maybe 10-15 years at the most, I would say.
10-15 years would also be my guess. Hard to predict though.
Hi Mark
When have no distinction between science and science fiction; it undermines science.
Science is not whatever somebody pulls out of their butt.
Hi Alan,
I agree that we were just speculating. On my side, it is based on nothing. It is not science at all (again on my side). Just having fun. Maybe we should not do that here. I’ll try to be more careful.
Hi Aldebaran,
Maybe science fiction is great. The problem for me is when “leaders” in anti-aging talk science fiction and act like doing something other than wild speculation about new advances.
This is blog. It is expected people say any crazy stuff they want to. I was referring to “leaders” who get widely quoted by media.
Don’t be careful Aldebaran, we’re all just having fun here, and who knows, today’s science fiction may be tomorrow’s science.
Alan,
I see your point. When leaders presents science fiction as science then I agree that this is undermining science.
Hi Paul,
I am not always sure where to put the limit. So let’s have fun as long as it is clear from the context that we are just speculating.
For me, good science fiction is about possibilities that you cannot refute while science is about possibilities that you can achieve. In some cases, I agree that it is hard to draw the limit between the two.
Yes I get carried away sometimes with speculation (sorry, Alan), but I made a concrete prediction about mice lifespans. We shall she is my hypothesis is correct. That is science.
Alan:
I do not think Einstein agreed with you.
Here is what Einstein said about imagination:
“Imagination is more important than knowledge. For knowledge is limited, whereas imagination embraces the entire world, stimulating progress, giving birth to evolution.”
-Albert Einstein, What Life Means to Einstein
I hate to admit it here but I spend most of my life , and even most of my everyday, immersed in speculation, and not really in science. I am constantly speculating about the existence of an afterlife and God, the origins of consciousness, the morality of eating meat, perhaps the possibility that I’m wasting my life trying to live longer, and why am I trying to live longer, is it just fear of the void, the horror of an eternal nothingness. In fact I speculate about practically everything. I exist somewhere between science and speculation at all times. It’s part of what separates us as humans.
So on the subject of speculation, what other pathways other than the insulin/MTOR/AMPK pathway might we intervene with, in the pursuit of defeating aging?
The above pathway I think of as the calorie restriction (CR) pathway. It contains elements of MTOR inhibition, AMPK activation, autophagy and mitophagy. It even protects telomeres to some extent (discovered recently through TERRA).
Are there any other important anti aging pathways?
Heat and Cold treatment spring to mind. Telomerase elongation is another pathway.
Have any supplements or medications been shown to reverse any other epigenetic changes associated with aging?
Any substances that inhibit senescence through a non CR pathway?
Ways to upregulate the Immune system?
Is there a place for sex hormone therapy?
Can we increase subcutaneous fat (the good fat)?
Are any of the senolytic (senescent cell removal) candidates safe to take yet?
Or is it more efficient to intervene in the same CR pathway through multiple different avenues? For example enhanced AMPK activation in addition to MTOR inhibition. Or directly upregulating autophagy and mitophagy, to a greater extent than the CR pathway does on its own, or via another pathway?
Any thoughts welcome.
NAD+ and NADH manipulation
Klotho upregulation
And activating repair mechanism
(Example: a-msh analogs activating the MCR—1 which activates NER in keratinocyte, whitout them being exposed to uv) keratin plays an important role in protecting epithelial cells)
NAD+/NADH ratio upregulates fission and hence mitophagy, so this is affected by the CR pathway, although there is likely additional benefit to upregulating it directly. But I believe it also upregulates DNA repair, which is something different.
I believe klotho regulates insulin sensitivity, so that would be the same CR pathway, though I could be wrong.
Can you tell me more about the MCR gene and how to upregulate it?
With regard to the NAD+/NADH ratio, does anyone know about betalapachone – I had it
synthesized – and its effect on the NQO1 gene?
I gave David Sinclair a 97% pure sample. He called it a “very interesting” substance.
Ooops replied to you below Mark.
Isn’t C60 the wildest speculative compound we currently have? Do we even have any idea of how it could possibly impact aging?
Yes I’ve tried it, and my best guess based on the one rat study they did, is that it is an extraordinarily powerful antioxidant, which locates to the mitochondria. It may have other mechanisms too. I certainly found it to help me recover from workouts quicker, and it seemed to offer some protection from alcohol, which is consistent with it being a mitochondrial antioxidant. I’ve sometimes found it to make me tired, particularly if I dosed it too regularly, so I’m wondering if it can trigger mitophagy.
Unfortunately it is currently mired in controversy over whether it protects from cancer or causes it, and the original 2012 study has never been replicated. I have a feeling there are complications between the effects of the C60 and the olive oil it bonds with. Plus rats and mice don’t do so well on high fat diets.
Thanks.
So it could be a super version of mitoQ. Certainly interesting to follow up.
Hi Mark
One pathway involves life extension in mice through fibroblast growth factor which is strongly induced by fasting, but no changes in AMPK, TOR, NAD, or sirtuins . Seems unique.No CR effect either.
The Starvation Hormone fibroblast growth factor extends lifespan in mice. Zhang. elife.2012 1: e00065
Reducing IGF-1 with metformin doesn’t need to involve AMPK,. Mice mutations with low IGF-1 live 25-60% longer than controls.
Brown-Borg Nature 1996 384:33 and Flurkey. Mech Aging Dev 2002 123 (2-3) 121-130
Reducing Angiotensin 2 , Enalapril prolonged life span in rats by 21%.
Histone Acetylation and deacetylation with phytochemicals and supplements. Great discussion on this : antiagingfirewalls 2009/05/30 Giuliano and Watson
Rifampin in synergy with rapamycin extend yeast and fruitflies. Mechanism of rifampin not as a CR mimetic
Hi Mark, Paul,
Very interesting discussion.
Question are they additive ?
If additive, excellent opportunity.
If not additive, maybe some common final pathway.
Or if not additive, maybe some unknown wall.
You’d think that they would be additive but I have this great idea. Why don’t you add rifampin to your regimen and report back in 6 months. If at that time you’re cycling 2000 miles; I’ll try it.
Hi Paul,
Thanks;
But not on Blagosklonny list of anti-aging meds; so I’ll pass.
Hi Paul,
Very interesting statement of how your brain works. This is not matter of intelligence as you are very intelligent person. A matter of how brain hard wired. My brain automatically rejects everything that not true by predominance of evidence. Even as a child although raised in traditional religious home, I dismissed idea of God and afterlife as nonsense and never revisited question. So just matter of how wired. I just never consider things that I consider not supported by facts.
Hi Alan
I can respect that. I have a philosophy degree so my thoughts go all over the place, but I must admit that fear of death motivates many of my musings.
I do not understand those that fear death. I see death as a new beginning (NOT in the sense of personal life after death). I don’t want to die only because others would suffer.
Hi Florentin,
Part I don’t understand is why you want to live past 30 or 50 or maybe 21; why pick 70?
Hi Florentin
How is eternal nothingness a new beginning?
Well your own death is not something you are going to experience, so it’s nothing to fear. Dying is another matter. As is the death of your loved ones.
I am guessing Alan, that Florentine is very young, and 70 is sufficiently abstracted not to mean anything.
Hi Florentin:
I am glad you do not fear death.
I am, personally somewhat conflicted.
I like to say I do not fear death, but only the pain of dying.
But there are so many questions. I think fear of the unknown is a normal part of being human.
I really fear walking through a dark cave without a flashlight and a rope attached to me to guide me back out, if things get weird.
I think that is probably really how I feel about death. It is such an unknown.
I would not mind a swift and merciful death. …at least that is what I like to think.
As for life being a new beginning, I think that is a possibility. Perhaps it is a passage into another dimension.
If there is a new beginning, things could get interesting. If there is nothing….I guess we likely will not know there is nothing.
Just lights out.
I studied Zen for fifteen years, and still have an interest in philosophy, particularly the eastern ones, and also stoicism. But I do resent how Zen has been used by modern culture and even used as an excuse to embrace death. A Zen monk would live an austere existence, but with a rich inner life. In many ways a recipe for a healthy, long and happy life.
In terms of your suggestions Paul, I’m afraid we can’t separate intermittent fasting benefits from CR, and IGF is too intertwined with MTOR for us to be confident benefits would be additive. I regard angiotensin treatment as mainly benefiting mitochondria. So it probably wouldn’t sum if you’re already doing NR or something like that.
HDAC inhibitors are very interesting. Some are clearly linked to CR or mitochondria and even telomeres. It would fascinating to unlock these mechanisms. Would be great if there a supplement that could keep all the chromatin as it was when you were young. I’ll give that article a read, thanks.
I also have a look into riframpin.
See rapamycin with rifampin and allantoin in synergy to increase lifespan of yeast.
Hi Mark
You seem like a ZenMaster. I’ve always wanted to go to Bhutan, the Buddhist kingdom, maybe next year.
Thanks Paul, if only!
I do think the benefits of meditation for health and lifespan are real. Josh is of the opinion aging is driven from the brain. I think this might be going about far, but I can certainly agree the brain can accelerate aging. Therefore finding inner peace could conceivably reduce the toll of aging through the mechanism of stress reduction and possibly other pathways too.
Dear Alan, interesting, but what are facts? Things we accept given our current ability to understand them? How many things that are “facts” today were throught to be ridiculous, impossible, and not supported by “facts” at previous points in time? Do you really think we are nearing some pinnacle of knowledge now? Wont someone look back on this 100 years from now and laugh? Respectfully, Erik
Hi Erik,
I am guessing that 100 years from now, many will laugh about how long it has taken us to consider aging as a disease.
Yes, I agree! Since others have mentioned Einstein as the greatest scientist ever (I wont debate that), we know that he denied that black holes were possible as late as 1939, 78 years ago. He changed his mind later of course, when he had more “facts”/data.
Hi Erik:
There are a lot impressive creative scientists. I quoted Einstein because of the “imagination” component.
Paul mentioned Tesla and he is one of my favorites. A very creative adventurous thinker.
Unfortunately he did not play politics well and was overshadowed by Edison.
Yes to all, we could list so many, the work of Luther Burbank fascinates me still. And to clarify, I did not mean to point out Einstein’s humanness, as all great scientists will take a blind path at some point. I was only was using it as an example to refer back to the post about never revisiting the idea of God because there is nothing “factual”. Do we know what we think we know? It quickly become philosophical as I think Paul mentioned.
Dear Josh,
Any thoughts on how this recent paper on chromatin silencing related to exercise or other supplement therapies? https://www.ncbi.nlm.nih.gov/pubmed/29073021
Let’s let Alan try it first like he did rapamycin.
Hi Heather
Nice Einstein quote. Greatest scientist ever. Not even close.
A couple of unrelated things that are interesting. I remember a study several years ago that showed that just measuring the pace of walking is very predictive of overall mortality rates over a 10 year period. People who walked at a slow pace had a significantly increased mortality rate. Even dementia. They defined slow as greater than a 24 minute mile. Plos One 2013 (8) 11. They claimed that not much else is more predictive of mortality.
Don’t know if you’ve ever had your IGF-1 level checked. Seems like a good idea. Both high and low levels are bad.
Mine came back as 149ng/ml. It’s surprising that there’s no general agreement about the optimal level. So I took a look at 28 studies and read Dr. Fuhrman’s comments on the subject. The average western diet leads to a level of 200-210 in that population. Vegans tend to be under 150. Over 200 and under 85 both lead to significant increased risk of cancer, CVD and overall mortality risk.
Should shoot for under 175, even more protection under 150, and at my age the perfect number is 130. I’ll have to try metformin.
IGF-1 is sort of like TOR except that unlike TOR it has the good sense to diminish wit age.
Yes IGF-1 is an interesting one. I expect it reduces as a protection against aging by slowing everything down, though this is me speculating again.
I was thinking about cellular senescence the other day, and it occurred to me that cells are arrested all the time, say due to replication errors, or damage from ROS. When this happens there is effectively a battle between catabolism and anabolism – AMPK and FOXO (triggering autophagy)vs. MTOR and P21 (trying to continue growth and degrading mitos further). Unless the former can hold out long enough for DNA repair to be completed the cell will permanently become senescent, and there’s no way back from that (without telomerase or epigenetic reprogramming). So we can immediately see the importance of keeping low MTOR and ROS, and high AMPK, and possibly better DNA repair too. I think this process is happening all the time, with MTOR mainly winning, and it is just the robustness of the youthful immune system that removes this constant loss of functional to senescent cells. With time this changes in favour of senescent cell accumulation, and by the time this causes inflammation to rise too high, we get stem cell and telomere dysfunction too.
I think you’re right , it’s constant antagonism between the forces of growth and those involved in slowing it all down. TOR and IGF seem to win in the end leading to senescence and inflammation. Aging.
Which is why we need to intervene, especially with rapamycin,metformin,immune modulators and anti-inflammatories.
Hi Paul,
In regard to walking speed in old people.
If walk slower than 1.8 mph decreased survival. My guess if live in NYC and walk slower than 1.8 mph you are going to road kill when try to cross the street. On other hand if walk faster than 2.3 mph good chance can make across the street.
Hi Paul:
I appreciate your input. Thank you for the information about the optimal IGF -1 levels. Very helpful to know.
I do not eat flesh foods, and have not since age 16, after seeing a documentary on how they slaughter animals, so that may help keep IGF-1 lower.
The walking information is interesting, too. Some people are forever telling me, I walk too fast and that I need to slow down, but I can not seem to comfortably walk slowly.
I wonder if talking slowly, independent of an exognenous head injury, or a recent vascular event in the brain, is also predictive of Alzheimers or dementia and earlier mortality?
Were you able to get a recent measurement on your ejection fraction?
What dosage of Metformin are you considering taking?
Hi Heather
Your IGF is probably good. Two things seem to bring it up in almost equal fashion, animal proteins and refined carbohydrates. I do eat fish and chicken but no refined carbohydrates to speak of, so maybe I should start substituting pea protein for the chicken at least.
As for metformin, the more I read about it the more I like it, but I’ll start with 250mg and work my way up, while trying the b12 that you recommended. Need my insulin at 5 and IGF at 130.
Keep walking fast. Highly predictive.
So I was so aggravated at my idiot doctor that I forgot to get the referral for the echo. So I’m just going to go soon and pay for it. Lol
Sorry to hear that your doc would not give you the referral.
I also end up paying for a lot of testing on my own.
My health insurance is rarely used because it will not pay for the type of testing I want independent of an obvious disorder or disease.
IMO, It’s good to start low with the Metformin.
I started low and slowly went higher but I did not want to lower my HgbA1C too much because too low is not good either.
My HgbA1C was already in range and went to the lower healthy range with a small dosage of Metformin.
I did some experimentation and settled on 125 mgs in the a.m. and 125 mgs in the p.m. This keeps my HgbA1C at a healthy level.
I split a scored 250 mg tablet.
I like the metformin dose and HbA1c is better than FBS that’s for sure. Not sure what’s too low. Maybe < 5
What would be bad about a low HGHA1b? Would it indicate too much insulin is produced?
Hi Aldebaran,
Hypoglycemia is bad.
Need to maintain normal glucose level 24 hours. Brain needs glucose.
Low HdA1c would indicate chronic hypoglycemia .
You can easily look up long list of things that could cause hypoglycemia.
Hi Alan,
Thanks. You are right. I was not aware about chronic hypoglycemia. I have done a quick lookup and found the following possible causes. Interesting.
– Excessive alcohol consumption.
– Liver hepatitis
– Kidney disorders
– Insulin overproduction (due to tumor of the pancreas and/or enlargement of beta cells of the pancreas)
– Hormone deficiencies.
Hi Paul:
Endocrinolgists now think a good Hemoglobin A1c range for a NON-diabetic is between 4 to 5.9 percent.
I feel good at the lowest end, but some people feel good closer to 5 percent.
I was wondering, would anyone here be able to give me some advice on arrhythmia? My Dad (77) was suffering from occassional dizziness and has been diagnised with this condtion. His specialist is currently considering the option of a pacemaker. I do not have information on his medication at this time apart from knowing he has been on statins. He walks a lot, and does portion control with meals and has managed to keep his weight from rising too much. He does drink however. Many thanks in advance for any advice.
Hi Mark,
Anti-aging is about prevention not treatment established disease. Advice about arrhythmia is follow advice of cardiologist. If uncertain get second opinion of another cardiologist. Also worthwhile to travel 1000 miles to see leading cardiologist at best hospital.
Mark:
I agree that he needs to work with a cardiologist, to identify location and type of arrhythmia, but a cardiologist that is open and friendly to nutritional supplements.
If he is taking a Statin drug and he is not already taking the Ubiquinol form of CoQ 10, he should find a doctor that will help him add it.
Some statins deplete CoQ10
The ubiquinol form is absorbed much more efficiently that ubiquinone form.
Nutrients known to stabilize heart rhythms are epa/dha, acetly l Carnitine, Taurine, and he may need magnesium, potassium or other minerals.
If he is not taking a blood thinner, Nattokinase to prevent clotting may help.
Berberine is beneficial for ventricular arrhythmias due to lack of oxygen.
All of this should be done under guidance of a MD with knowledge of nutritional support for heart health and can run blood testing for deficiencies.
Thank you both for your advice.
In light of the fact there is a lot of users of rapamycin in here, what are your thoughts of this:
https://www.youtube.com/watch?time_continue=18&v=pSU96tdQSp4
TLDR: CR = increase and self renewal of Intestinal stem cells
Rapamycin = blocks the renewal of intestinal stem cells because of the inhibition of mTORC1
(I will get back to you in regards to MCR1 a little later mark).
Was the rapamycin low dose weekly?
atleast supplementation with nad+ increasing compounds should not be taking at the same time as rapamycin, and i am really considering if a weekly dose of rapamycin is the best approach, i would consider longer time in between.
This is a bit odd. Both CR and rapamycin will slow proliferation, but end up preserving stem cell function because they reduce senescence. Like you Paul, I can only imagine the rapamycin dose was not intermittent. I’ll watch the video through though, to see what they say.
Hi Mark,
Rapamycin has been in clinical use for 18 years and used on over a million paper. The one thing we have learned if nothing else is all about DOSE. CR only has low dose as regards inhibition of mTOR. Rapamycin is a poison in high dose, so people can show high dose poison all day long and means nothing to me. What means something is studies to show how to best use Rapamycin to achieve best anti-aging effect.
Also anything meaningful should be in form of paper published in scientific journal .
Hi alan
heres your paper:
https://www.ncbi.nlm.nih.gov/pubmed/27345368
I don’t understand your methodology, when looking at rapamycin. I can assure you that rapamycin is no panacea. Why not look at the data and relate to it?
Example: Metformin
Pros: DNA Methylation, Cancer Chemopreventative, Anti-diabetic
Cons: lactic acid
solution: creatine, omega-3 magnesium
Example: Rapamycin
Pros: mTORc1 inhibition
Cons: interferes with the positive effects on Sirt1 on ICS
solution: space apart your Sirt1 activators (resveratrol, pterostilbene, whatever) apart.
I dont now why you perceive anything negative about rapamycin as pseudoscience.
Thanks for posting paper.
Well known CR and Rapamycin different.
Effect CR is to lower mTOR and increase Sirt1. Effect on Rapamycin is only reduce mTOR and no effect Sirt1. This study used sirt1 knock out mice and showed different effect.
Benefits Rapamycin stand on their own evidence and nothing to do with CR.
So anybody likes 30% CR, welcome to it.
Agreed incorrect to say Rapamycin is CR mimetic. Rapamycin is Rapamycin, not CR.
If you want to knock intermittent use of Rapamycin, present some evidence about intermittent use of Rapamycin.
You presented good study to show Rapamycin different from CR; so what.
I have been on intermittent Rapamycin for about 2 years with excellent results and very much like effect and how feel on Rapamycin. It is a mild feel good drug.
I could last about 2 days on 30% CR, maybe if got paid enough money each day.
CR has been known to be beneficial for 100 years; but extremely few people opt for 30% CR.
Hi
Your points are interesting and deserving of further research. I wasn’t aware of the sirt1 issue until now, so perhaps as you suggest when I take rapamycin on a Sunday I should wait until Tuesday or Wednesday to hit the resveratrol/ pterostilbene. That’s certainly a consideration. Will look into it.
As far as metformin is concerned, the incidence of lactic acidosis is so rare that we’re wondering if it’s even from the metformin.
Hi Paul,
Phenformin caused lactic acidosis.
Metformin used by more than 100 million people and one of safest drugs in world; although some non-diabetic very sensitive as you well know and could become symptomatic from mild hypoglycemia.
Only issue with metformin is only indirect effect mTOR.
I take metformin for mitochondria and anti-cancer effect.
However, study which showed diabetics on metformin lived longer than non-diabetic was extraordinary finding.
As regards SIrt1, in study with angiotensin2 blockers, increased rat lifespan ( normotensive rats) and one effect was on Sirt1 plus mitochondria.
So right, increasing sirt1 is excellent, but not action of Rapamycin.
Sure thing!
I am not trying to knock intermittent rapamycin, in fact i think it is a great ressource.
I am trying to solve the issues at hand, and finding out what the best approach is , and the only way to do that is to look at the studies/evidence.
yes you are correct Paul, i just used lactic acid as an example. I should have used the homocysteine/b12 deficiency instead, which is in fact a real issue.
my best
I think to really compare CR and rapamycin properly, you’d have to work out the exact severity of CR required to cause the same reduction in MTOR given by the dose of rapamycin. I suspect rapamycin is a much more potent MTOR inhibitor that all but the severest CR, so most comparisons of different gene expression changes are not 100% valid. I’m not saying they are the same thing, bit they’re probably not as different as this study is suggesting. Anyway, as stated by many commentators previously, mitochondria should be protected by other interventions, as well as the benefit to mitochondria from rapamycin.
Hi Mark,
One great difference CR and Rapamycin was CR only increased lifespan when started early in life. Huge surprise with Rapamycin was increased lifespan when started middle age mice.
In Blagsklonny theory, aging Hyperfunction and stimulation growth stem cells is fundamental problem as drives production senescent cells. However, not stimulating stem cells can help preserve stem cells.
Main thing, need a theory of aging to interpret results as good or bad.
Very unclear to look at individual results.
The question is did those acts slow aging and increase lifespan.
I wonder Alan, is there much advantage in starting rapamycin early, or can you get the full benefits in terms of lifespan starting at, say, 60?
Hi Erik
Now that I think about it, Tesla is right up there with him. That guy was damn smart
I would put Godel and Turing in the same division.
And don’t forget Newton, Pasteur, and Edison
Definitely.
Maybe Yamanaka could be one of them if epigenetic reprogramming turns out to be the next big thing in anti-aging.
Forgot about Godel. Good friends with Einstein. Studied Kant and Husserl, a phenomenologist, believed in God and wrote an ontological proof of God. I never could comprehend one single word of his incompleteness theorem. Not a word.
He has discovered some fundamental limits to the axiomatizability of mathematics. He was pretty good in philosophy and even made significant contributions in theoretical physics (probably from is relations with Einstein).
Yes, he basically proved there are theorems that are unprovable.
For those who like gossip.The above you tube video features Leonard Guarente,
whom I have known and interviewed since 2006. As he begins his lecture he refers
to two students of his at MIT, Brian Kennedy and Nic Astriaco. I have interviewed
both of them. Nic left his fellowship in the UK in the 90’s after 9 months and entered the priesthood. He now teaches genetics at Providence College and also consults
on the ethical issues brought up by research. His long ago partner, Brian Kennedy,
was actually his mentor when he returned to research after being ordained. Kennedy
recounted that first meeting “Nic came in with his clerical collar and his bible and we trashed it out, argued our positions” – all done in understatement. Guarente explained that when he told his colleagues about Nic entering the seminary, their reaction was
“worse than if he had died.” Lenny and Brian have clashed over their dueling genes,
srituins and mtor, on and off for years.
Very interesting, thanks. Personalities shouldn’t matter in research, but they do!
Hi Robert:
So, research scared him into priesthood.
Research is so political that I can somewhat see how thought priesthood was a better choice.
Maybe the church can you this as a marketing tool.
And a female. Marie Curie
And an Ancient Greek. Aristotle
Greek were great philosophers and great mathematicians. In particular, they made the fantastic discovery that the square root of 2 cannot be a rational number. Probably the first mathematical proof by contradiction in the history.
https://www.math.utah.edu/~pa/math/q1.html
Yes. And we should include Michael Faraday
And Maxwell as well since we are in the electromagnetism.
Don’t know much about Turing except the nazi code stuff
Alan Turing has, among other things contributed to formalized the concept of computability (what functions can be computed by a machine). He has discovered a model of abstract computer (called Turing’s machine) which is heavily used in theoretical computer science and complexity theory. He is also known for his work in AI and in particular for having invented the “Turing test” to decide about the intelligence of machines.
Hi Aldebaran,
All these comments about great thinkers; but it is the DOOFUS who makes the world what it is. WW1, WW2, and upcoming WW3, it is the Doofus that allows the totally unfit to gain great power and cause the hundreds of millions of lost lives in past 100 years.
After a short period of enlightenment,; then we plunge into the age of Doofus.
And let’s not forget the Quantum Physics pioneers, without which the modern world of silicon chips, transistors, etc., could not exist and we would not be able to have this conversation: Bohr, Schrödinger, Heisenberg and Bohm.
Hi Alan,
Possibly the DOOFUS are ruling the world but I don’t have a good answer to that. I can only quote Churchill: “Democracy is the worst form of government, except for all the others”
Thanks Aldebaran,
I certainly agree Maxwell great scientist; but I live in Doofus land.
Hi Aldebaran
I’ve been unable to find anything so far about hba1c being ever too low. Maybe Heather will clarify
Hi Paul,
Thanks for looking at that!
I am really curious because I have never seen anywhere that having a low HBA1C could be an issue.
Hi Aldebaran
Always a pleasure.
Back to one of our prior discussions let’s say that the average lifespan is 80 ( I don’t know what it is)
It’s possible that with good genes and strict lifestyle I could make it to 95 or so in pretty good health, let’s just say no major problems.
I now introduce rapamycin into the equation. What now would be an acceptable result?
Let’s say 100 in pretty good health. No
How about 100 in really good health, vital and robust. Yes
How about 105 in pretty good health? Again Yes
110 in poor health? No
What’s your take?
Hi Paul,
So let’s speculate. Rapa add 10% max LS in mice when started in mid life so in theory (assuming same ratio) 105 in good health would seems possible to me. Pretty good right?
110 in poor health No? It depends I guess. If health started to decline at 105 it is not that bad. Plus, you would have your name listed as one of the very few super-centenarians in the world!
Another possibility is that rapa buy you the time to reach the next anti-aging treatment when you are 100 and then you make it to 120 healthy. So thanks to Rapa, you have lived 25 more healthy years even though Rapa itself have only contributed to 10. How about that?
Well Aldebaran it’s hard to argue with your very logical mathematical mind.
I like option 1. Being 105 in good health is good stuff. I’ll take it.
Option 2. Don’t love it, but I guess in the context of getting first to 105 and then 10 bad years, maybe. I don’t like the headline:
” He died at 110 frail, sickly, and miserable, but he made it”
Option 3. My favorite. Get to 100 and then super technology give another 20. Perfect!
One thing that should give us hope, is that the centenarians and super centenarians were NOT in good health, they just had the right genes to limp on with a large senescent cell burden and huge fused mitochondria. We will hopefully be preventing these accumulations so we should be at minimum very healthy until near the point when we die, and then depending on our genetics we’ll then limp on too, or quickly succumb. It’s hard to say what age that would be but I’d be surprised if it’s younger than 90 for an average person without any particularly bad (APOE4) or good (FOXO3) genes. And then like Aldebaran says, we’re only 10 years from very effective senolytics treatment (or sooner if you travel abroad but take the risk with it being unregulated). I’d say the time scales for telomerase therapy and maybe epigenetic reprogramming are not that much further out.
Hi Mark,
I think you mischaracterize many centenarians. My understanding is many reach age 100 in excellent shape and then die very quickly. Nobody does autopsy when die at age 101. I have no idea why they die. What kills 100 y/o can be very different than what 80 y/o die from.
So big question is what kills healthy centenarians.
Mouse studies didn’t help as mice die same thing (cancer) just older age.
Maybe acute mitochondrial failure as in mitochondria paper you posted about 3 months ago. Remember big holes mitochondrial membrane.
I agree they are healthy compared to their compatriots, but I don’t regard them as healthy. I think the mitochondrial membrane pore is the mechanism by which cells carry out apoptosis, at the behest of the mitochondria who dump their innards out into the cell prompting the nucleus to order self destruct. I think those that reach very old age have not only a naturally low MTOR, but probably also a natural resistance to apoptosis. This might mean some get cancer earlier in life, or perhaps they’re protected from cancer too by low MTOR or other mechanisms. I’ve heard that the very old often die of transthretin amyloid build up in the heart. But they also have very few remaining stem cells, according to the analysis of the blood of one, so they might be coming up against replicative senesnce too.
Thanks to Mark, I went to Telocyte’s website and read Blasco paper about telomerase gene therapy in mice. Results looks really interesting when applied at mice of 1 year or 2 years old. Having said that, I am wondering why no other studies have been published since 2012.
Telocyte is now trying to tackle Alzheimer disease with the same approach. They think rescuing microglial cells by inserting extra copy of HTERT will cure Alzheimer. Obviously, this is a very very ambitious goal.
Assuming that they have the funding for their clinical trial, I am wondering what could be the schedule. I would think:
2018: phase 0 (animal model)
2019: phase 1
2020-2022: phase 2 (is 2 years reasonable?)
I see 3 scenarios for phase 2 ( I am assuming it can measure efficacy to some degree, even if not statistically powered for that):
– poor results or high toxicity: end of story
– mixed results (no clear improvement but trend toward improvement): could be hard to find funding for phase 3 so the situation is unclear.
– good results: this is a revolutionary finding Company is bought or funded by major actor. Phase 3 start ASAP (or maybe FDA could even approve therapy based on phase 2). Other trials for other aging diseases are started. Anti-aging as a whole is acknowledged as a valid approach.
Am I out of reality or does this seems reasonable? What could be the chances for a good result after phase 2? Any speculative bet?
Hi I Aldebaran,
AD is 2 hot disease with first hit being severe damage to micro vascular system.
Second hit is amyloid cascDe with Tau.
Late problem is microfilm activation which causes chronic inflammation which causes more damage.
Want to lower activity microfilm not increase, but this late stage and will not help.
I rate their chance for success less than zero.
Hi Alan, The CEO of company knows that; only the rubes buying the stock don’t. Name game is hype the product, sell stock to the suckers believe this will cure AD. LOL
Hi Alan,
I cannot argue with your expertise. Good to have your opinion about that. Thanks.
This is Michael Fossel you are talking about Alan, Telocyte is not a con. He has intentionally selected a trial on full blown, not early onset, Alzheimer’s to blow the whole FDA stance on aging wide open. Plus Alzheimer’s is basically the most horrible disease of aging. His approach is diametrically opposite to yours Alan because he is trying to restore gene expression to youthful levels, which entails some speeding things up, notably the metabolic digestion of aggregate proteins by glial cells, which is where his confidence comes from that this will work. He is aiming to start trials next year, but this is dependent on the FDA accepting some of Blasco’s mouse work.
Incidentally Aldebaran, she’s done lots more studies since 2012, including work on pulmonary embolism and seeing if telomerase activation makes pre existing cancer worse (it didn’t), and also activating some of the shelterin telomere proteins and seeing how they preserve telomere length. All her work is using mice but is aimed and translating to humans.
Hi Mark,
I agree with you.
Approach 100% different.
I consider treatment of AD when have dementia plaques and tangles impossible.
If you think might work, I’ll give you 5:1 odds on a friendly 1 million dollar bet.
However, apoe4 carriers have changes in PET scan 50 years before onset dementia at mean age 75.
And those people can be treated before onset of disease.
If works in E4 nice and more likely than not work in human carriers ApoE4.
That treatment for apoe4 carrier will be available very soon.
Hi Mark,
Putting Tellorite aside.
As regards biotech start up companies as a generic group.
Does you agree that purpose of company is to sell stock based of the scam that they will have a great drug.
Hi Mark,
Thanks for pointing out the more recent works from Blasco. I will look at it. Regardless of its applicability to Alzheimer, I have found the mice study of 2012 convincing.
I agree that pharmaceutical companies in general cannot be trusted, but Michael Fossel is a guy like yourself who would ordinarily be thinking about retirement, and has no need to do this for money, but I believe genuinely wants to make a difference. I think he has a fair shot at success, and I would take you up on your bet if I had a cool million to spare! But that also doesn’t mean I don’t think your approach at prevention would not work. So far pharmaceutical companies have not managed prevention or cure! Although thinking about it, the ‘failed’ recent trial that cleared amyloid beta but did not improve symptoms probably would work as a vaccine.
I’m glad you are becoming a fan of Blasco Aldebaran!
And imagine – the results she got in the study you’ve seen was from only a single intervention AND done in mice who don’t get diseases of short telomeres like humans do.
Hi Alan,
I agree that the purpose of biotech companies is to make money, whether they have a useful drug or not. From time to time, a few turn out to have a useful drug. For example, I am thinking of CAR-T (Kite, Juno). But no doubt there are lots of scam out there.
Mark,
To me, the 2012 Blasco study looks very interesting. However, I am not familiar with gene therapy so I am more in a learning mode here. Of particular interest, multiple measures of aging improved in the 2 mTERT groups compare to the other groups (control and eGFP group): decreased p16 levels, decreased short telomeres, increased bone density, decreased insulin levels,…). Life span increase was significant in both 1y and 2y groups.
I am wondering if CRISPR technology could improve the efficiency of the therapy and reduce off-target. Also, I am wondering if this therapy reduces mTOR levels. Maybe it could also affect some epigenetic markers.
Hi Alan,
I have a question for you. Suppose you have a great preventive treatment for Alzheimer but you need to start it very early (40 years old for example). On which basis can FDA approves it? Could PET scan be convincing enough? Animal models? Obviously trials cannot measure success on AD itself right?
Thanks,
Hi Aldebaran
If brand name drug and unlimited millions, very easy.
Only people at risk E4 carriers and study treatment only for them.
Use PET scan for glucose metabolism.
Also PETs an for amyloidBeta.
Also clinical testing memory.
However, because generic no money for tests.
Only way is off label.
Note E4 have 2-3 times the risk and onset 10 years sooner.
Hi Aldebaran,
Blasco uses a viral delivery to express HTERT within cells for a transient effect extending telomeres. It is not integrated within the genome so it does not become permanent. CRISPR would no doubt make a permanent change, which we probably wouldn’t want.
The work showed longer telomeres improves the health and lifespan of mice, which was surprising to some given the length of their telomeres, but agrees with the in vitro work by Shay and Wright showing gene expression changes as telomeres shorten. Interestingly this ties in roughly with expected lifespan: mice telomeres are 3 times longer than humans but shorten 90 times faster, so they live up to around 3 years rather than our 90. This much greater rate of telomere shortening is set by their much higher rate of MTOR, and probably much higher ROS too, which isn’t sufficently compensated for by their longer telomeres and active TERT (hence the benefits of the treatment). It is exactly the same problem we’ve been lookong at with CR and rapamycin, etc., but looked at from the other side.
Actually, slight modifier, mice don’t generally suffer from replicative senescence so the rate of shortening can’t be x90 humans. It must be considerably less than this because they can undergo 4 generations with no TERT before they get short telomere diseases like humans. But DNA replication errors and ROS produce a lot of senescence anyway. And extending telomeres in mice helps avert both this, and the changes of gene expression that cause other problems.
Hi Paul:
There are studies that suggest that Hba1c increases “all cause mortality” when too low.
Note the journal article discusses low cholesterol in people with TOO low Hba1c.
The Mayo clinic states that very low levels of LDL cholesterol may be associated with an increased risk of: Cancer. Hemorrhagic stroke.
According to the journal article, this increase in all cause mortality occurs both in NON diabetics as well as diabetics although the range is different for the non-diabetics and diabetics.
In normal people and Hba1c level below 4 in some research is shown to be detrimental.
http://circoutcomes.ahajournals.org/content/3/6/661.long
From the link:
[ “Participants with a low HbA1c (<4.0%) had the highest levels of mean red blood cell volume, ferritin, and liver enzymes and the lowest levels of mean total cholesterol and diastolic blood pressure compared with their counterparts with HbA1c levels between 4.0% and 6.4%.
An HbA1c <4.0% versus 5.0% to 5.4% was associated with an increased risk of all-cause mortality (HR, 3.73; 95% CI, 1.45 to 9.63) after adjustment for age, race-ethnicity, and sex.
This association was attenuated but remained statistically significant after further multivariable adjustment for lifestyle, cardiovascular factors, metabolic factors, red blood cell indices, iron storage indices, and liver function indices (HR, 2.90; 95% CI, 1.25 to 6.76).
Conclusions— In this nationally representative cohort, low HbA1c was associated with increased all-cause mortality among US adults without diabetes.
Additional research is needed to confirm these results and identify potential mechanisms that may be underlying this association." ]
Dr Brand
Check out ” Sirt1 negatively regulates mTOR”. Ghosh 2010 5(2) Plos One
So it would seem by this study that:
CR and resveratrol induce SIRT1 activity and levels. Resveratrol activates sirt1 which then inhibits mTOR, mediated through TSC2.
Insulin and IGF lower SIRT1 levels, thus raising TOR levels.
CR, resveratrol, and rapamycin all inhibit m TOR, all protect against age-related disease, and all induce autophagy as well as inhibit senescence.
So actually if you use them all at once you’ll blast TOR pretty good and seemingly in an additive manner.
B12 deficiency is a real issue with metformin in about 10%. High enough .
This makes sense Paul, i am all in for inhibiting mTOR in a intermittent fashion. I was merely pointing out that based on the study we see:
sirt1 activation + mTOR activation –> increased stem cells
sirt1 activation + inhibiting mTOR activation –> no increase in stem cells
This is in mouse, we simply dont no if it applies to humans.
One could still use the sirt activating substances on Rapadays considering they still provide antioxidant activity and so on.
This also fits when considering that mTOR is a driver of Growth, it would make sense for it to play a role in the growth/rejuvenation of old and new stem cells.
On another note, i am not a fan of CR i believe IF is far superior.
This is based on the fact that IF continues to drive down insulin where CR does lower insulin levels it does plateau.
When CR is compared with IF in regards to lower body fat % IF is also better then CR but only marginally, but IF does twice as well in regards to where it matters the most, the fat around the stomach.
Another concern is that “fasting will significantly burn muscle mass” but in fact it turns out that IF preserves muscle mass 4 times better then CR.
In addition to this fasting triggers pathways that does simply do not get switched on by “only” doing CR.
I could see CR being superior to IF in regards to total amount of mTOR activation but this is just speculation and i could see the opposite too.
– brand
According to Blagosklonny aging theory mTOR drives aging and age related disease.
MTOR driving growth causes resting cells to become senescent cells.
So Rapamycin is used to reduce mTOR to reduce Hyperfunction and mTOR driving growth.
In regard to great minds noted in previous comments; I would place Blagosklonny on same level as Charles Darwin.
Problem is, everybody wants to be an Indian Chief and everybody has their own theory.
Hi Dr Brand,
Thanks for this interesting information. I am aware that mice on high fat diet live longer with resveratrol but I think mice on standard diet do not. In theory, we would expect SIRT1 activation to significantly increase life span so I am wondering if resveratrol should be combined with something else to be more effective.
Regarding IF, in addition to the many health benefits that you have mentioned, do we have also data showing significant life span extension in animal models?
Thanks
Paul,
You raise an interesting point that resveratrol, rapamycin and CR might synergistically inhibit mTOR. I am not sure if this has been tested on mice but it would probably be worth doing the experiment.
I think we all believe that inhibiting mTORc1 is good.
I just think that we need to look at the bigger picture also, stem cells play a vital role In this picture. I want to live a long life, but i would prefer it to be a healthy one too. I want to be 110 but it would be wonderful to look and feel like 60 at 110 too.
This reminds me of the greek myth of Tithonus, Eos, Goddess of the Dawn fell in love with Tithonus a merely mortal prince of Troy. Eos asked zeus to grant Tithonus immortality, which Zeus complied to, but Eos forgot to ask Zeus to grant Tithonus eternal youth so as timed passed he became a stain on the floor unable to move. Later though he got turned into a cricket.
Regarding resveratrol, i don’t think it is the best candidate for sirtuin activation, it only activates sirtuin1 and it has a awful bioavailability (did they inject the mouse or did they feed them orally?) further more we see that there is other problems too like rapid metabolism and elimination.
I would like to see a study on stable sulforaphane which activates NQ01 this increases nad+ and nad+ activates all of the sirtuins 1-7, furthermore we see that sulforaphane has an BA at 80% and a much higher CD value. CD value of sulforaphane is 105-fold greater than resveratrol.
“Given that oral doses appear to be capable of increasing NQO1, we consider whether it may be possible that a sulforaphane-yielding broccoli sprout powder might deliver a plasma concentration of ~2.00 μM. By calculation, a 1% powder yields 56.4 μmol sulforaphane per gram. Ye et al. showed that a single 200 μmol dose resulted in a peak plasma concentration of ~2.0 μM after 1 hour. As Ye et al. [159] had shown that a 200 μmol oral dose had resulted in a plasma concentration of ~2.0 μM and Riedl et al. [160] had shown that 102 μmol had increased NQO1 mRNA expression by ~200%; these orders of magnitude could be achievable with a sulforaphane-yielding broccoli sprout powder. Theoretically and by calculation, an individual could consume around 2 grams of a 1% sulforaphane-yielding broccoli sprout powder to achieve what Riedl et al. achieved with 200-gram broccoli homogenate and 4 grams to achieve what Ye et al. achieved with a single 200 μmol dose.”
“Sulforaphane and Other Nutrigenomic Nrf2 Activators: Can the Clinician’s Expectation Be Matched by the Reality?”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4736808/
Dr. Brand you are on a good track using Sulforaphane to upregulated NQO1 a more sustainable way to upregulate NAD+. Plus as you rightly pointed out it’s activates the very powerful Nrf2 which has many beneficial actions one of which is inhibiting mTOR. There is SulforaDex the only stable Sulforaphane provider I have found. I had read somewhere that it’s better than taking the broccoli sprouts powder as some issue was pointed out about that source if you Google you should land on the one I came across.
Transresveratrol increases bioavailability of some nutrients it’s taken with. Another alternative is Pterostilbene which has much better stats then Resveratrol and is the one Guarante used in his NR pill to improve it’s bioavailability and efficacy.
I will add pterostilbene to my NR.
I found a stable supplier of Sulforaphane their product is called prostaphane and is made by a french company.
I saw in an earlier thread that you showed interest for GHK, could you elaborate a bit? have you tried it?
I started collecting notes on GHK glycyl-L-histidyl-L-lysine after Broad Institute (collaboration of Harvard and MIT) singled it for resetting of genes to a more healthier state.
In human plasma, the level of GHK-Cu is about 200 µg/ml at age 20. By the age of 60, the level drops to 80 µg/ml.
I am unable to quote study titles so please Google GHK and Broad Institute. Sharing some part of a research article by Loren Pickett published in BioMed Research International – it’s open access:
numerous studies over the course of four decades demonstrated that this simple molecule improves wound healing and tissue regeneration (skin, hair follicles, bones, stomach, intestinal linings, and liver), increases collagen and glycosaminoglycans, stimulates synthesis of decorin, increases angiogenesis, and nerve outgrowth; possesses antioxidant and anti-inflammatory effects, and increases cellular stemness and the secretion of trophic factors by mesenchymal stem cells. GHK’s actions on gene expression were determined by the Broad Institute and, using their data, we determined that GHK increased or decreased gene expression (UP or DOWN more than 50%) in 32.1% of the human genes. In a recent gene study, the Broad Institute’s Connectivity Map was used to find potential therapeutic agents for aggressive, metastatic colon cancer. The gene analysis computer program selected GHK from 1,309 bioactive molecules as the best choice to reset the diseased gene patterns to a healthier pattern.
Another study says GHK, abundantly available at low cost in bulk quantities, is a potential treatment for a variety of disease conditions associated with aging. The molecule is very safe and no issues have ever arisen during its use as a skin cosmetic or in human wound healing studies. Thus, GHK would be expected to influence the cells’ gene expression to be more similar to that of a person of age 20–25, an age when the afflictions of aging are very rare. Based on our studies, in which GHK was injected intraperitoneally once daily to induce systemic wound healing throughout the body, we estimate about 100–200 mgs of GHK will produce therapeutic actions in humans. But even this may overestimate the necessary effective dosage of the molecule. Most cultured cells respond maximally to GHK at 1 nanoM. GHK has a half-life of about 0.5 to 1 hour in plasma and two subsequent tissue repair studies in rats found that injecting GHK intraperitoneally 10 times daily lowered the necessary dosage by approximately 100-fold in contrast to our earlier studies.
This should get you started.
Wow Akshay, GHK sounds remarkable! Have you tried it?
Also, do you have any useful information on honokiol and magnolol, two active components of magnolia I’m looking into right now?
Mark,
My Lab is awaiting committee approval to launch a double blind placebo trial with GHK on rats. We are including a very comprehensive list of assays to thoroughly investigate its efficacy besides safety and dosage. If successful we will apply for human clinical trial next year.
This is what I have in my notes on Honokiol and Magnolia derived from studies:
Honokiol is known to induce an antianxiety effect and magnolol is considered to be an antidepressant.
Research has clearly shown that honokiol is able to stimulate the release of acetylcholine and inhibit the action of acetylcholinesterase
Various observations have revealed the protective role of the honokiol molecule vis-a-vis the mitochondria in the cells of the brain, liver and heart. Honokiol protects these vital organs from the harmful effects of free radicals. In its role as a powerful antioxidant, honokiol has a unique capacity to prevent the peroxidation of lipids, a primary risk factor for cardiovascular disease.
Finally, another important virtue of honokiol is its ability to normalize blood glucose levels. It has been convincingly shown that the honokiol molecule can reduce blood sugar levels and prevent weight gain in diabetic mice. This is due to its agonist action vis-à-vis the gamma PPAR
(peroxisome proliferator-activated receptor), which are proteins of the nuclear receptor group, liaison, lipids and transcription of target genes involved in adipogenesis and metabolism. As an agonist, honokiol mimics the action of these PPAR and has a similar physiological action that can limit the production of adipose tissue and fat accumulation in adipocytes.
The use of an extract of Magnolia as a complement to food should not cause any health related side effects if the prescribed doses and treatment instructions are strictly observed. The recommended daily dose is between 30 and 90 mg per day. It is recommended that extract of Magnolia capsules be taken at mealtime.
Purchasing a standardized Magnolia extract with a purity rating of more than 90% is the best way to maximize the benefits of honokiol.
Combination of honokiol with the mTOR inhibitor rapamycin presents synergistic effects on induction of apoptosis of cancer cells.
Hi Akshay,
GHK looks remarkable. How long will the mice study take? Which endpoints are you going to measure? Looking forward to see the results!
Thanks
We hope to wrap it up by end of January 2018. We will be comparing 7 end points.
Great stuff Akshay, looking forward to hearing more once you’ve got your rat trial results.
This sentence stood out for me in your description of GHK: ‘GHK increased or decreased gene expression (UP or DOWN more than 50%) in 32.1% of the human genes.’
32.1%!
If this is confirmed this molecule will be of great importance in the fight against aging.
Thanks also for your comments on the extracts of magnolia, I am thinking of using it instead of Berberine for glucose control. I am also interested in its potential for adipogenesis (the subcutaneous, anti inflammatory kind). The only thing that remains as a question mark in my mind is the fact that honokiol can protect mitochondria, but also increase membrane permeability and cause apoptosis in cancer cells (via the transition pore). Here is the relevant study.
‘Honokiol induces a necrotic cell death through the mitochondrial permeability transition pore’.
So yet another molecule doing one thing to cancer, and another in normal cells.
Yes Mark and thanks. I would lean towards honokiol vs magnonol.
Hi Mark,
Your comments about BENEFITS of subcutaneous adipose tissue of are very interesting. I consider subcutaneous adipose tissue on arms and legs neutral as opposed to visceral adipose tissue.
I find your idea that can decease inflammation by increase of subcutaneous adipose tissue a very novel idea. Furthermore, since in humans, excess fat is generally stored as as midline abdominal fat, doesn’t seem any way to increase subcutaneous fat beyond normal physiologic amount, without increasing abdominal fat. In short, you seem to be proposing something which as far as I know, is impossible.
Do you have any evidence for this idea in a paper in a science journal.
Hello Dr Brand,
In regard to Greek myth, it is current traditional medicine which aims to keep very sick people alive, demented people in nursing homes, respirators, feeding tubes etc. Anti-aging medicine aims to slow aging and prevent age related disease, like dementia. I see extension of lifespan as only a secondary side effect; if people are healthy then would live longer.
I have been researching this for a while as a possible anti-aging strategy and have gathered evidence that subcutaneous fat is GOOD, anti-inflammatory and insulin sensitizing through the action of the adiponectin receptor. Consider the health of a child and also consider how very early in adulthood much subcutaneous fat is LOST. This appears to be one of the earliest signs of aging and is visible in the face even your 30s. For background on health benefits see free paper ‘Adiponectin Receptor as a Key Player in Healthy Longevity and Obesity-Related Diseases’.
The strongest evidence however comes from a paper on the treatment of diabetics with pioglitazone. Look up free paper ‘Pioglitazone Increases the Proportion of Small Cells in Human abdominal Subcutaneous adipose Tissue’. The diabetic subjects got fatter (without any increase of visceral fat) but healthier, according to markers of insulin resistance.
Unfortunately pioglitazone is (weakly) associated with bladder cancer with long term use, look up free paper ‘Pioglitazone use and risk of bladder cancer: population based cohort study’. Although risk only increases from ~0.9% to 1.2% with over 2 years of use, and limiting factor that all users were diabetic, and other meta-studies have found no association, I believe small risk is probably real. PPAR gamma activation, which is causing desired adipogenesis is also active in the urinary bladder. So if one was to use pioglitazone, would have to use it for very limited period and have good cancer preventative regime in place. For more information see free paper ‘Deciphering the Roles of Thiazolidinediones and PPAR𝛾 in Bladder Cancer’.
As an alternative to pioglitazone the active ingredients of magnolia (particularly magnolol) have shown ability to increase adipogenesis in human adipose mesenchymal stem cells, at least in vitro. See free paper ‘Magnoliae officinalis extracts promote adiponectin production during adipogenesis in human adipose tissue-mesenchymal stem cells’.
You are very sharp to pick up on my passing comment Alan, and I would value your opinion and input on this possible intervention.
Hi Mark,
My analysis study,
Used overweight/obese people with high level insulin resistance.
Drug promotes PPARG which promotes creation new fat cells.
My guess fat people have feedback loop inhibition PPARG so don’t make new fat cells just make bigger fat cells.
Piog stimulates PPARG so make new fat cells and fat people able to redistribute so have more small young cells and less old big cells in visceral fat.
Net effect is without weight loss fat people reduce insulin resistance.
Also small fat cells may be ones make
Adiponectin which agree good.
My take, good for fat people.
My treatment plan: loose 50 pounds.
That is best way have insulin sensitivity.
When want to loose 50 pounds want low level PPARG.
Note this was study on fat people.
You is not fat person. You have healthy amount SC adipose tissue and don’t need any more.
However, I can now see how plio can work for diabetic fat people. So learned a lot from paper.
As regards 20 y/o with loss baby fat, that is not aging. That is very healthy fit people with low percent body fat. That is what healthy athletes look like.
Check out level body fat on worlds top men tennis players. That is good health.
I get your point Alan that the easiest way to have insulin sensitivity is to remain slim. As you point out with athletes such as tennis players, often the slimmer the better. It is certainly the case that the very long lived are always very slim for their age. This is the current state of our longevity efforts.
However I am looking to the future when we will look not only to live a long time looking almost like an marathon runner, where we are fit and healthy in spite of being old, but actually start looking young again, and having the innate health that comes from not being old (biologically). The very young often look like they are fatter, but it is really just puppy fat and is part of what makes them so healthy. They remain insulin sensitive even on a diet of junk. And they exercise only for fun, they are naturally active because it feels good to move, but they do not really need to, and it does not tire them in the same way it does later in life. This is a new avenue I think we should begin to think about and investigate and it is what I have been attempting to look into.
Some very interesting thoughts Brand.
It is my impression that lessening the population of senescent cells through TOR inhibition is good for all cell populations, including stem cells, but if you’re right that would certainly be a point against rapamycin. But I don’t think so.
Great ideas about IF vs. CR. We know that with chronic low energy intake that the body responds with an equal degree of decreased energy expenditure, in other words a drop in metabolic rate , which does not occur with IF.
Also IF leads to a pronounced decrease in PCSK-9 which dramatically lowers LDL cholesterol and is the mechanism of the new monoclonal antibodies to prevent heart attacks. IF is safer and cheaper than the new drugs, and even more effective.
I agree with the limits of BA with resveratrol. I think pterostilbene is better. Great info on sulforaphane, I didn’t know about the sirtuin connection. I eat broc sprouts and the freeze dried ones. Akshay likes a pill, sulforadex, but I can’t find it.
Sub-q fat is bad, but not as bad as visceral fat which is in close proximity to the portal vein and this gives those nasty inflammatory chemicals a direct shot to the whole body. Also, Sumu wrestlers have enormous sub-q fat but virtually no visceral fat, so the two aren’t necessarily correlated.
Good EOS story!
I’m glad that two of the avenues I’m currently investigating have just been mentioned by others – NF2 pathways and increasing subcutaneous fat! I am convinced these are pathways that will sum with both MTOR inhibition and mitophagy and i’m working on solutions to both, although the subcutaneous fat increasing option might have some risk (so I’d be curious how the Sumo wrestlers do it!)
What do you think of Brand’s comment that rapamycin may have a detrimental effect on stem cells? Have you heard of that before Mark?
Hi Paul,
That is exactly what Rapamycin supposed to do.
MTOR drives growth
Rapamycin decrease stimulation to grow.
Stimulation to grow results in senescent cells.
Slow stimulation, preserve stem cells.
That is Rapamycin effect.
Hi Alan
My thinking is in line with yours but it seems like he’s saying that by slowing growth one would also be impairing the growth of stem cells. I think that that is similar to the thinking that rapamycin would impair the development of the immune system until it was found, in intermittent doses, to have the opposite effect.
Hi Paul,
After 6 months on Rapamycin had decrease hemoglobin, lymphocytes and polys as reported. This due to putting brake on hematopoietic stem cells. Mild anemia very common effect.
I consider this benevolent side effect and helps protect stem cells from development senescent cells which much bigger problem.
So slight inhibition stem cells real and probably part of anti-aging effect.
Yes it is unclear whether this would be good or bad in vivo. Echoing what Alan said, obviously blocking protein synthesis includes sirtuins, but it’s only intermittent so would take this finding with a pinch of salt, and obviously whatever the downsides of rapamycin, it extends lifespan in everything it’s been tried in.
Hi Alan
I too have had a slight decrease in WBC’s after 3 months
Hi Paul,
After initial decline leveled off and few values increased. Most still in normal range.
On flip side, if develop senescent lymphocyte, could provoke damaging chronic inflammation.
Plan is to preserve stem cells for future.
Sumu:
High calorie diet, 5-7000/day.
Low in sugar and processed foods.
Intense exercise schedule leading to elevated adiponectin levels and insulin sensitivity.
Low cholesterol, triglycerides, and glucose levels.
Low visceral fat and ceramides ( toxic lipids)
So virtually all of their protection is secondary to their exercise regimen and adiponectins. Once they retire, it’s rapidly down hill.
You’d think the big amounts of subcutaneous fat would give them some protection, but I guess without the exercise a similar calorific intake would add a lot of visceral fat.
Agreed. And we also don’t know if they start eating junk.
Maria Blasco has a PHD in molecular biology and is the director of The Cancer Research Center in Spain. It was primarily reading her work that convinced me to take TA 65for 3 years, and now a group of other telomerase activators. My real concern was that it may convert an insolent cancer into a more aggressive form, but she put those fears to rest. I’m never certain why Elizabeth Blackburn and others just sort of ignore her findings. She’s totally legit.
Hi Paul,
Just regarding price, availability and status of telemere related products and saying nothing about merits, my understanding is as follows:
TA-65, $600 month, 250 units, food supp
Other drugs that Mark has been talking about:
Not on market, will require FDA approval, phase 2 human trials not yet begun; probable time to market, over 5 years, probable cost, high.
Are there any other natural supp cost @ $25 a month
Replied below.
Hi Alan
There have always been several knocks on TA 65, jusitfied or not. One is cost. They blame that on the cost of extraction.
The other is efficacy in people. It seems to work somewhat in mice ( Blasco) but not like rapamycin, Also there have been actual human studies showing elongation of the critically short telomeres.
The main knock is regarding safety and cancer risk mainly because scientists like Blackburn and DelPinho keep saying it, and have from the beginning. Even Vince, a very early and ardent proponent stopped it over those concerns. Do they know something? I doubt it.
Totally agree, her work is brilliant. I guess Blackburn prefers science to stay theoretical and never actually benefit anyone.
I like Elizabeth Blackburn. After winning a Nobel prize she remained a scientist. She could have made millions becoming a pitchman. So I like scientists. I have nothing against entreupeneurs. However, I Have great suspicion of scientist turned businessman. I also believe ZERO of what businessman says about their product.
So unless somebody with no financial ties to company verifies data; to me have nothing.
I still remember how all CEOs in cigarette industry said…
And business people haven’t gotten any more honest in fifty years.
So I believe Elizabeth Blackburn.
Well she helped found the company Telome Health Inc. where test kits were sold for about $200. Not totally pure
Looks like strength training shouldn’t be ignored. A very recent study out of Sydney looked at 80000 people and found that twice a week strength training of any sort reduced all cause mortality by23% and cancer deaths by 31%,while aerobic training had more of an effect on heart disease.
Journal of Epidemiology 2017 Stomatakis et. al.
Telomere Plus from enzymedica has been subjectively good for me. Cheaper not to buy it from their website (around 20 sterling from amazon). As for scientific evidence read this paper, ‘Identification_of_Telomerase-activating_Blends_From_Naturally_Occurring_Compounds’.
Although this study was paid for by the manufacturers for the cell type they looked at the results seem impressive. And the natural substances used all have decent bioavailability, unlike cycloastranagol.
As Alan says we’ll have to wait for a safe viral vector and gene therapy to have telomeres extended significantly, but we might not need to wait for FDA approval. Just look at Bioviva’s website. These guys look like they are setting up clinics as we speak, the price will presumably start very high and then come down to more realistic levels.
I’ll check it out. I guess ideally you should get a full blown telomere analysis at baseline and then keep repeating it to see if the pills are having an effect.
On that note, too bad we can’t directly measure mTOR levels somehow.
We do know that telomerase activators elongate telomeres but do we know if they impact life span of animal models? In her 2012 paper Blasco was saying:
“Telomerase activators have been reported (de Jesus et al, 2011; Fauce et al, 2008; Harley et al, 2011), however, their mechanism of action is still poorly understood. Instead, we turned into a TERT-based gene therapy strategy to extend longevity, to our knowledge unprecedented in the context of aging studies. “
I think telomerase activators only gave a healthspan increase in mice, whereas the gene therapy increased mean and max lifespan.
Cycloastranagol has a terrible bioavailability (although better in mice than in humans). In any case it clearly isn’t strong enough to give the effect we’re looking for.
Comments from Micheal Fossel about BioViva:
http://www.michaelfossel.com/blog/?p=139
“For another thing, Liz knew that our biotech firm, Telocyte, intends to do almost the same thing, but with a few crucial differences: we will only be using telomerase (hTERT) and we intend to pursue human trials that have FDA clearance, have full IRB agreement, and meet GMP (“Good Medical Production”) standards.”
Incidentally, BioViva has in its pipeline several other potential therapies (than telomerase). I am wondering if they have the funds to really explore all of these. Part of it could be marketing but I really don’t know.
It is hard to say, but Liz is an excellent speaker and is always on the road, so I wouldn’t be surprised if they get the funds together to open some clinics. We should know in a year if this is going to happen.
Looking at Blackburn 2017 book; no commercial endorsements.
In regard section on testing she lists no companies and adds as caveat unregulated business.
Didn’t find her name linked to any commercial enterprise.
Everything in book to maintain telomeres is free.
So looks to me like unlike very many others, Blackburn retains her scientist standing and is a very credible expert.
Liz is definitely a good speaker and I hope she will get the funding she needs. However, I don’t like too much idea of creating a clinic offshore without the proper trials.
Given the number of parameters that improved in mice in the Blasco study, (BMD, insulin, memory, …), it looks feasible to me (although certainly expensive) to establish the same improvements in humans in a relatively short time (3-5 years). That could give them a lot more credibility.
FDA approval could be more complicated because they need to target one disease in particular though, and they would probably need to focus on a very serious disease to justify gene therapy.
I think Liz’s argument is that the FDA route is flawed because it 1) Takes too long whilst patients are dying now, 2) Still results in many withdrawn drugs, 3) Is too expensive to pursue for all but the biggest Pharma companies, AND 4) Results in very expensive treatments (to recoup those costs).
She is calling for a more risk balanced approach. Best of all she is honest that there are risks, and has put her own life on the line with the first treatment.
Hi Aldebaran,
Fascinating stuff, off shore treatments, gene treatments.
So I looked BioViva and first picture I saw was Aubrey De Grey. Since to me De Grey and that whole crew are nut cases; count me out.
Hi Mark,
I understand her point that the FDA route is flawed but BioViva does not have to go through FDA approval to validate its technology. They just need to fund independent placebo-control studies. I think it is unavoidable at some point for BioViva’s credibility. In any case, I hope she’ll succeed.
Hi Alan,
I know that Aubrey has not a lot of credibility in your mind but don’t you think that the technology itself, as demonstrated by Blasco in several mice studies, is really promising?
Hi Aldebaran,
I think Blasco work has great potential.
However, gene therapy is very novel never used before. Therefore, any gene therapy should go through normal channels FDA approval.
Approval by FDA would be great.
Bypassing FDA to set up gene therapy on Fiji looks like what somebody called regarding this “new low medical quackery”.
So Blasco, great, act like a scientist, do the studies, present to FDA.
Treat in Fiji, looks like bunch nuts risking lives of people with more money than brains
Well the FDA has started to approve gene therapies now, although only for specific maladies, not aging itself, which might be a bit of a leap for them. That another reason why Michael Fossel is going the FDA route with this therapy for Alzheimer’s. Liz is going the other way, off shore – less credible, but faster and cheaper. It will be interesting to see which approach will be more successful. If Liz gets some success with undeniable results (like an obviously rejuvenated person according to many biomarkers), then the game will change and it might even be curtains for the FDA.
“Curtains for FDA” The FDA is medicine’s defense from quackery. FDA not involved in anti-aging and so have field totally over run by quack medicine and quacks.
Quack medicine very toxic and absence of FDA is sorely missed.
Yes we need a defence against quackery as you put it, but the current system cannot remain in place. The regulatory burden has resulted in a vested interest system when only multi-billion dollar companies can even consider investing in a new treatment, and would only do so if the returns look good enough. Such companies are actually opposed to any in kind of rejuvenation of aged people, because it would reduce the health care burden, and hence their profits. The whole system needs shaking up and re-baselining, with a sensible risk of treatment vs. risk of delaying treatment approach. That is not to say I think there should be no regulation. The problem is, what government agency, whose job is to regulate, would willing regulate less? We shall see, but if they do nothing and refuse to change we do risk a off shore free-for-all.
Hi Mark,
The great problem is translation from basic science to clinical medicine. I think system works very well for new brand name drugs. Big pharma happy to spend few hundred million on clinical trials and have billions in profits.
Gilead curing Hep C and near cure of AIDS is extraordinary success story.
True that system doesn’t work for generic drugs, but they can be used off label.
However, I greatly prefer FDA over anarchy.
The big problem is one thing humans are really great at is being liars and cheats.
I am of course very interested in telomere extension therapies, but the question remains, will this restore a healthy ‘young’ phenotype by itself?
Michael Fossel and Bioviva argue that it may well do that. But if senescence is not reversible and SC’s are not cleared, how will a healthy non inflammatory phenotype be restored?
If the main cause of cell sen. in humans is telomere attrition we may need some form of telomere restoration therapy, but perhaps, once it has occurred, only an effective senolytic can ‘turn’ the clock back by clearing SC’s (which just itself may cause as much cell senescence is the existing tissue has to replicate to make up for the loss).
All the super positive info about telemerase comes from people in business of selling stock in their telemetry companies.
One big infomercial.
Like to see any credible evidence from someone who doesn’t have huge financial interest into putting out BS.
The work with mice from Blasco looks very promising, so this is not just hype.
I am not sure if telomere elongation on its own can rescue senescence cells, although it has been done in progeria afflicted cells. I suspect it can. Perhaps also a rejuvenated immune system would increase the natural clearance post treatment. And if this is not sufficient perhaps a synergistic pairing would be senolytic clearance followed by telomerase therapy; as you say this might be necessary anyway as one will need to replace the removed senescent cells.
Hi Mark,
As I have an anti-aging medical practice with Rapamycin as cornerstone of treatment; I would be most delighted to be able to add an injection therapy which was approved by FDA.
I will believe when I see it and not before.
Glad to see GHK enter the discussion. I tried to post about it a day or two ago but none of my attempted posts show up. Not sure which ‘rule of engagement’ I keep breaking (?)
hi aldebaran
My ferritin level was 88 at last checked. I want it as low as I can get it without having iron deficiency anemia. My Hct is 48 with a normal MCH and MCHC. As long as those are ok then you’re fine , though some include a TIBC which I find redundant to the ferritin level which I feel is best. If you’re over 200 donate blood and start IP6.
Hi Paul,
Mine was around 140 last time I checked so it is lower than 200. The hypothesis that ASA is beneficial because of associated blood loss is certainly interesting and merits further investigation. However, I have not been able to find any evidence that ferritin lower than 100 is beneficial. I have only found evidence that ferritin above 200 is detrimental. Do you have more data?
I will start on IP6 regardless of ferritin level, as you have rightly pointed out that there is evidence for cancer prevention.
Thanks
Sorry Paul what is Hct?
Got it hematocrit! Mine is low so no issue on that part.
Sorry. I need to be clearer and avoid the medical jargon
Hi Aldebaran
Are you going to start donating blood now?
Hi Paul,
Ferritin is elevated due to disease, obesity, chronic inflammation, cancer, liver disease.,alcoholism Lots of things unrelated to iron. So agree low fetritin reassuring; but high fetritin, should see Internist.
I wrote a short article based on a recent paper by Leo Zacharski, in which he calculated that a normal ferritin, that is, one that is not associated with any form of ill health, is no more than 100. http://roguehealthandfitness.com/the-normal-value-iron-matters/
Hi P.D Magnan,
Thanks for pointing out your article. I was not aware of Zacharski study. I will read both your article and Zacharski paper with interest.
Hi P.D.
Ferritin looks like could be useful marker for both response to treatment and screen test for risk of disease.
Will consider adding ferritin to regime.
Thanks
Thanks for chiming in with that article. As usual we fail to measure the important things like insulin, IGF, and ferritin
Josh mentioned in his latest post that NSAID’s reduce cancer risk and that Celebrex may be the safest. Carlos has referred on several occasions to his studies on digoxin as cancer preventative.
A new study today in Nature Biomedical Engineering (Backman) used partial wave spectroscopic microscopy to look at chromatin in cancer cells. This revealed that a more heterogeneous and disordered chromatin packing density was related to greater cancer cell survival whereas a more ordered packing density lead to greater cell death with chemo.
They then combined digoxin with Celebrex, which they referred to as chromatin protection therapeutics, and these drugs restructured the chromatin so that every single cancer cell died because they could not respond to the chemo.
This worked in all cancers that they tried it on. Very promising.
Yes indeed. Good share Paul.
On your last post you wrote about another cardiac glycoside, Proscillaridin A, which must be in the same class of drugs as digoxin, and would probably do the same thing.
There seems to be a consistent pattern here with both cancer and aging – that a therapeutic is making the cells respond in a certain way, which makes them resistant to the changes induced by aging or cancer. That this mechanisms would be via epigenetics makes total sense.
For example, in vitro immortalized cells gradually gain methylation, but this primarily occurs on inactive gene sites. If the area of the genome is in use then it is maintained and far more resistant to methylation and deactivation. It takes many population doublings (>100) before active sites start to get methylated (in vitro). This can explain why exercise, calorie restriction and certain supplements work – by forcing an certain cellular response that is resistance to drift.
Thymosin β4 reduces senescence of endothelial progenitor cells via the PI3K/Akt/eNOS signal transduction pathway.
https://www.ncbi.nlm.nih.gov/pubmed/23151623
worth a look
interesting molecule, studien it further does however lead me to believe its anti aging purposes are, limited. Could be useful in a healing setting though.
This one will interest people into C60 oil:
Fullerenes as Anti-Aging Antioxidants
http://www.eurekaselect.com/145681/article
Mark suggests that much of its benefits may be from the rather potent antioxidant effect. The abstract seems to support this. Was that the bottom line?
Can’t get access to this unfortunately, but from the abstract they seem to be focusing on the mitochondrial uncoupling mechanism. Basically the C60 molecule transports protons within the mitochondria so lowering the membrane potential and decreasing ROS (and therefore aging). This seems to explain the recovery benefits users have noticed with exercise.
I’m not sure if this can explain the lifespan benefits of the Baati study, however. There might also be a permanent anti-inflammatory effect, due to accumulation in the spleen, as shown by the same study.
Richard Morimoto spoke today about his new study out of Northwestern:
Mitochondrial stress enhances resilience, protects aging cells and delays risk for disease. Cell Reports. Nov7
Using C elegant they screened 22000 genes and identified the mitochondrial electron transport chain as a central regulator of age related decline. They found that signals from mildly stressed mitochondria prevent the failure of proteostasis in the cell that comes with age.
“This has not been seen before. People have always known that prolonged mitochondrial stress can be deleterious, but we discovered that when you stress mitochondria just a little, the mitochondrial stress signal is interpreted by the cell as a survival strategy. It makes the animals completely stress resistant and doubles their lifespan. It’s like magic.”
Yes Paul, you catched the gist form the abstract.
That is a very interesting study you just posed, do you think metformins interference with mitochondrial complex 1 woud fall into the category of “mild stess”?
Metformin and Berberine both interfere with the electron transport chain, which then triggers AMPK. It is difficult to say how much of their resulting benefit is due to increased mitophagy (the stress part) or MTOR inhibition. I suspect it’s both but have never seen this proven.
Hi Mark
Your comments on fat deposits are pretty original. Concerning body fat, 90% of fat is subcutaneous, 10% is visceral. Visceral fat acts as an endocrine organ and gives off the very inflammatory cytokines, they also produce precursors to angiotensin ( another aging pathway), and lastly they produce retinal-binding proteins which increase insulin resistance (RBP4). They are developing a blood test for rbp4 it’s so linked to visceral fat.
As you suggest, subcutaneous fat is a different animal and produces both leptin and adiponectin to control appetite and reduce body fat.
So you’re on the right track. It is true that we lose ” baby fat” as we age. Do you have any theories about it ?
My best guess is failure of adipose stem cells to differentiate as they should. I am not sure why this happens so much earlier than in stem cells elsewhere in the body, but maybe it is because oxidation stress is much higher in the skin that elsewhere.
This is definitely a feature of aging. Just look at anyone in their 40s. Even if they take very good care of themselves you can tell they’re not 25. This is the main reason.
Hence plastic surgeons and juvederm injections
This is an interesting field, i believe that subcutaneous fat is very important. If we approach this from an Aesthetic point, what we see is that in older people their faces starts to change dramatically, this is mostly because of the loss of subcutaneous fat, and less with loss of elastin/collagen = wrinkles. offcoruse the two are interconnected. This is also why PRP and fat grafting is getting so much attention in skin rejuvenation atm.
I believe the one major reason for subcutaneous fat loss is because of loss of angiogenesis, the fat simply does not get the needed blood an nutrition. This is a two-way street, i believe that angiogenesis is good in some settings and really bad in others. (ex. cancer).
There is an animal study that suggest that PRP could be used to recover stem cells from senescence:
“Delayed animal aging through the recovery of stem cell senescence by platelet rich plasma”
There also is a lot of data on how rich subcutaneous fat is in stem cells.
to tie this to rapamycin, there is studies conducted with a rapamycin 1% topical formulation to inhibit the regrowth of telangiectasia in vivo (mouse and man) after laser treatment, rapamycin proved to be very effective at this, it is normally a pretty hard task. This makes me believe that rapa is a potent anti-angiogenesis agent.
Mark you asked earlier about the implications of using rapamycin before old age, again if we look at it from an Aesthetic point of view what we see in old age is the enlargement of nose, ears and hands, i believe this to be mainly driven by mTOR (and to some extent: HGH, IGF, Insulin), these changes is not something that happens overnight but is changes that occur over many years of increased mTOR, i believe that this increase/negative effect of mTOR begins already when you are fully grown, late 20’s early 30’s and at somepoint later in life really goes haywire.
Just my current conviction though.
Very interesting comment that old age enlargement nose, ears, hands due to increased activity MTOR, HCH, IGF.
I am just speculating here Paul, but i see it as highly plausible.
I actually like some aspects of Hgh not the synthetic kind (partly because of different actions but mostly because of halflife)
synthetic Hgh is around for way too long, it is this increased/sustained (over time) signaling from hgh to the liver that releases an abundance of IGF-1 not something that we want.
What we want is hgh to bind to its receptor, start its signaling cascade and vanish, not stay around too long and cause all kinds of havoc.
The way to do this is using a combination of:
GHRP/GHRH in 50mg/50mg or 100mg/100mg doses to stimulate the hypothalamus and pituitary to secrete gh. This should be done at nighttime, to simulate the natural release of the hormone. (in men, in women its different).
The preferred relasing agent (GHRP) is ipamorelin because it does not raise cortisol nor prolactin.
Currently i see the benefits of natrual released hgh (low dose, quick Metabolised) far outweighing the negatives.
The positives of hgh are well established.
Realease pattern of rHGH vs GHRP/GHRH:
This should not be done when rapamycin is most active in the system but should also be used in a intermittent manner.
The graph:
http://www.peptidequestions.com/wordpress/wp-content/uploads/2013/11/graph_daily.jpg
I feel that restoring subcutaneous fat to youthful levels is possible.
As for the other aesthetic or should I say, unaesthetic changes such as ear and nose growth due to protracted MTOR (and related hormones) activation, even rapamycin treatment will not reverse this, so the only option I can think of is surgery. So if we all live to 150, we’ll likely need to go under the knife at some point if we want to look young!
Hi Brand
You offer some interesting ideas. It is certainly becoming clear that a certain degree of mitochondrial stress is important and Mark is right that both metformin and berberine will do it, but they both have some associated negatives, but metformin at 250-500 a day seems ok. I wonder if a24hour fast with low dose metformin and exercise represents too much of a mitochondrial stress, or maybe just right, I suppose no one knows the sweet spot.
As far as C60 as a potent antioxidant, Mark has tried it, I have not, but I did do a self experiment 2 years ago. You are familiar of course with viagra which is a phosphodiesterase inhibitor and thus raises nitric oxide endothelial levels. This increase can also boost exercise endurance. So I took a pretty hefty dose and exercised with it, but then it always gave nasal congestion, headache, and flushing which I tried to eliminate with various high dose antioxidants. None of them worked at any dose except for one. Sangre de Drago is the highest rated antioxidant of any, with a sky high ORAC rating, and is literally blood red. In two minutes all of the nitric oxide effects completely vanished. It never failed.
Now Iget the same beneficial effects from pine bark extract 200mg a day without the side effects, but Dragon’s Blood was impressive stuff.
About the nose growth, the same holds with earlobes, and even though I like your theories, I think the simple answer is gravity.
On Nitric Oxide and Antioxidants the effect you describe is somewhat strange. I thought anti oxidants increased NO production? That said if Viagra is causing inflammation in addition to the NO effect then it is that the anti-oxidants are addressing.
I notice that many people use Sangre de Drago on wounds. I’ve used C60 in olive oil for this purpose and it works very well.
When you say the Pine Bark gives you the same effect, do you mean the benefits of increase nitric oxide (but presumably without the headaches)?
Your brilliant self experimentation has got me thinking Paul.
I love doing those sort of experiments, I’ve learnt a lot simply by playing around with cycling supplements or even simple dietary changes. Many of my discoveries have been accidental.
For example I have always suffered with hayfever and animal hair allergy which necessitated taking antihistamines. These gradually lose potency I have found. I took a 23andme test and found my body is particularly bad at using B6 (I inherited the less functional form of the gene from both parents). So I started supplementing it last summer. Low and behold I found my hayfever much improved and my animal hair allergy almost gone. I then looked into it and found B6 is required in processing histamine. How cool is that? I’ve made a number of discoveries like that, which have improved my life and health.
That’s remarkable Mark
Hi Mark
NO is a potential antioxidant, but it also acts as an oxidant , particularly in indirect reactions with oxygen or superoxide anion.
I love the B6 idea, my allergies drive me crazy and I avoid all antihistamines due to their anticholinergic effects which are linked to Alzheimer’s.
Some facts pertaining to Aspirin and Ibuprofen:
Aspirin:
It seems that a low dose of Aspirin in the range of 50 – 81 mg or even as low as 30 mg has the same anti-blodd-clotting effects as a normal to high dose of 300 – 1200 mg.
1) https://books.google.de/books?id=GnIQGmiSylkC&pg=PA1108&lpg=PA1108&dq=aspirin+75mg&source=bl&ots=iXpVbhuZQ7&sig=m1sJvOT_tDJzHXcony2F9MATen0&hl=de&sa=X&ved=0ahUKEwi01cuq_bDQAhVKDsAKHRMOAYY4ChDoAQhzMAM#v=onepage&q=aspirin%2075mg&f=false
2) https://www.ncbi.nlm.nih.gov/pubmed/4082090
3) https://www.ncbi.nlm.nih.gov/pubmed/10870801
Coated aspirin (protect) does NOT have the same effect as uncoated but is weaker
http://stroke.ahajournals.org/content/37/8/2153
Aspirin can help to reduce blood-pressure, but this effect only occurs when taken in the evening
http://www.docguide.com/administration-time-dependent-effects-aspirin-blood-pressure-untreated-hypertensive-patients
By the way, this time-dependent effect of drugs is commonplace and seems to occur basically with all drugs.
There are opinions that glycine uptake influences the precipitation rate of aspirin.
https://www.thieme-connect.com/products/ejournals/abstract/10.1055/s-2005-870853
Translation:
“Salicylic acids are coupled to glycine by peptides and as salicyluric acid renally eliminated. The precipitation rate ( rate at which a substance is removed from the body) at higher concentrations of aspirin is dependent on the amount of available glycine. One can suppose, that the uptake of glycine helps to lower the concentration of aspirin. Comparing examinations about effects and side effects should therefore orient themselves on the blood concentration and not the dosis uptake.”
As a side note:
This article claims that aspirin can even help women getting pregnant
http://www.mirror.co.uk/lifestyle/health/daily-aspirin-can-help-women-6672104
But this itself is not a study, but only a news article, so taken with care.
Ibuprofen:
Ibuprofen seems to have a slightly different set of attributes:
Anti- inflammatory ( like aspirin)
Pro- cardiovascular disease ( unlike aspirin)
https://www.ncbi.nlm.nih.gov/pubmed/24256349
a special pro-longevity effect (propietary)
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4270464/
So this effect seems to be based on to the inhibition of tryptophan uptake.
Combined uptake of aspirin and Ibuprofen:
Combined uptake of Ibuprofen is possible, but tricky and only sucessfull if done under a strict set of rules.
1) https://www.pharmazeutische-zeitung.de/index.php?id=pharm4_28_2004
2) https://ptaforum.pharmazeutische-zeitung.de/index.php?id=434
Google translate might be your friend here.
Summary:
1. One has to take the aspirin first.
2. the aspirin should NOT be of the coated ( protect) kind.
3. one has to wait at least 30 minutes after that before taking the ibuprofen, but also not longer than 2 hours.
4. the ibuprofen has to be weak, best not more than 200mg, even less is better.
5. only one ibuprofen per day allowed.
Under this circumstances can one reap the benefits of both NSAIDs. Discipline is mandatory, though.