

“Increased air pollution cuts victims’ lifespan by a decade, costing billions” blared the headline from Eurekalart last summer. I spent five months of the last 15 in Beijing, with arguably the worst air quality in the world. I call Philadelphia my home, with the 10th worst air pollution in the US. In the past, before good statistics were available, I have been an advocate, board member and even expert witness in support of clean air legislation. Now I dreaded discovering what air pollution might be doing to my long-term health. I procrastinated, and left this project on a back burner for a year. But when I finally chained myself to my desk to research this column, the results were not nearly so bad as my fears.
The above Eurekalert article referred to this research from Denmark, and the summary, it turned out was misleading. The question it appears to be asking is, “if you live in a city with 10μg per m3 of particulate pollution, how much sooner must you expect to die?” But in fact, it addresses a different question: “Assume that air pollution has zero effect on the great majority of people, and that the entire burden of increased mortality comes from a small number of unlucky people. If you are one of those unlucky people, how much is your life cut short because of air pollution?” (Even for this unrealistic assumption, I am not convinced that the author did the calculation correctly.)
For context, the study was based on the concentration of the smallest particulate pollution, particles less than 2.5μm in size, which are thought to do the most damage. A concentration of 10μg/m3 for such particles is a level typical of a large American city on an average day. Philadelphia has many days each year exceeding this level. Beijing air on a summer day has 150μg/m3, and winter days are typically 400-600μg. If my reading of the Danish study is correct, it implies that the average citizen of Beijing loses 500 years of life to air pollution.
Questions
Beginning my reading, here are the questions I was curious about:
- How much life is being lost to air pollution in American cities and Chinese cities?
- What pollutants are responsible?
- Is the risk linear with pollution, or is there a threshold?
- Are sources of pollution predominantly local or regional?
- Where are the best and worst places to live?
- What diseases are associated with air pollution?
- What can be done to mitigate health consequences of exposure to air pollution?
- Is it better to exercise in polluted air or not exercise at all?
I came away realizing that some of these questions are difficult to address with field studies and epidemiology, and others have not been addressed, even though they are not so difficult. But generally, I was re-assured that air pollution is not as big a health threat as headlines had led me to fear.
How big is the effect overall?
This study looked at day-to-day variations in death rates in Wuhan, a large, polluted city in China’s heartland. They find that 10% of all deaths are due to respiratory disease, and some large fraction of respiratory deaths are triggered by the day’s SO2 level. (Sulfur dioxide is a significant pollutant in China, but not America, because so much coal is burned in and near cities.) This speaks of the immediate effect only, and corresponds to less than one year of life lost. But this kind of study can tell us nothing about long-term effect. Another study in Eastern China (Jiangsu province) compares across cities, so is potentially sensitive to long-term as well as immediate effects. They find a smaller effect of ozone (O3), corresponding to a few months of lost life.
One of my first discoveries in researching an early ScienceBlog column five years ago was that large differences in mortality correspond to small differences in life expectancy. The deep cause of this counter-intuitive effect is the steep rise in mortality curves, building a wall of death into actuarial tables. This is what Benjamin Gompertz realized two centuries ago, but I was a little late to the party.
These mortality statistics are large enough to detect unambiguously, and a few percent increased mortality (up to 10% in China’s most polluted cities) sounds quite serious. But when these numbers are translated into life expectancy changes, the results are far less alarming. 10% in the worst Chinese cities corresponds to less than 1 year of life expectancy. 1% – 2% typical of American cities corresponds to about a month of life expectancy. Much more difficult to quantify is the extent to which the health effects of air pollution are focused on a subset of people who are particularly sensitive, and who will suffer a seriously early death. This is the question addressed by the headline-grabber I quoted at the top of this column [ref].
The most recent comparison of South and North China (where coal was burned freely for winter heat) is featured in Eurekalert with the sensational headline, Air Pollution Cuts 3 Years in Northern China, but the research article behind it reports 8 months.
My own informal study: Life Expectancy in American Cities
Can we see an effect of pollution on life expectancy in America’s largest cities? I looked up the data, and found a surprisingly large variation in life expectancy. Here is a scatterplot of life expectancy plotted against EPA’s measurement of average morning pollution levels for the smallest particles (PM2.5).
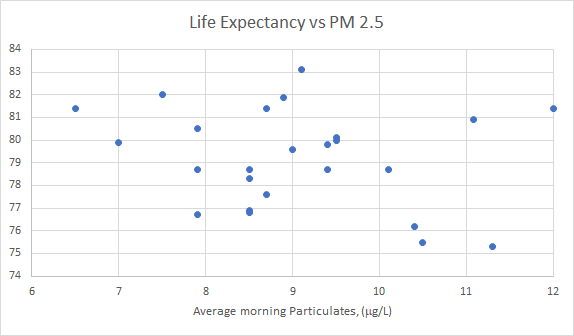
There is a correlation that goes in the expected direction, but not statistically significant, and no clear visible trend. For comparison, look at the plot of life expectancy vs per capita income:

Here there is a statistically significant correlation (p=0.01) and a trend that is visible to the eye. Across 25 cities, 29% of the variance in life expectancy can be explained by wealth alone.
[Source for pollution data]
[Source for life expectancy data]
[Source for income data]
Mechanism of long-term damage
When mice breathe air with particulate pollution, their arterial walls thicken and stiffen, arterial plaques increase, and inflammation rises over a period of months [ref]. Similar effects in humans would be expected to increase risk of heart disease and ischemic stroke. Much of this damage is thought to be reversible after ths source of the pollution is removed [ref].
Joel Schwartz of Harvard School of Public Health has persisted through a long career in creating some of the most solid and credible connections between pollution and its health consequences. This classic study, more than two decades old, uses conservative statistical methods to separate effects of weather from pollution. (Weather is known to be highly correlated with daily mortality, more so than pollution, and pollution, of course, is correlated with daily weather and also with season.) The result is a robust conclusion that TSP of 100 μg/m3 increases risk of death by a factor 1.06. The weakness of this finding is that, since the time of this study, TSP=“total suspended particulates” has gone out of fashion as a measure of pollution. TSP measures large particles more heavily than small, but we now know that the smallest particles are most damaging.
Air quality in America has improved in the last 20 years, and most days, most places are compliant with EPA limits. Nevertheless, a difference in mortality rates can be detected between the good days and the bad. A recent study from Schwartz’s group investigated the question of low-level pollutants. They are able to detect effects from three pollutants: PM2.5, O3 and NO2, and report a total ~1% increase in daily mortality.
Dose-Response
This is a large unanswered question, very difficult to pose in an epidemiological study design. It is plausible that high exposure for a short time is more damaging than low exposure for a longer time, but the opposite is possible. It is plausible that the combination of chemical irritants (e.g., O3, SO2, NO2 with micron-size particles is worse than either of the two separately, but we don’t know. A “latency” is often assumed, such that today’s exposure to bad air can produce hidden damage that shows up a decade later to cause disease or death. But it is just as plausible that those who are fortunate to escape disease in the immediate aftermath of pollution exposure suffer no long-term consequences. We do know that hospital admissions and both cardiovascular and pulmonary mortality rise in times of major pollution events. But smaller day-to-day fluctuations in air pollution also produce smaller fluctuations in a city’s mortality and morbidity rates, and these can be correlated in long-term studies.
Is there a threshold, below which low levels of pollutants cause no problem?
Probably not. This study by Schwartz found that 1% or 2% of all deaths in Boston are arguably attributed to particulate and ozone pollution, and Boston air is cleaner than most large American cities, and was within EPA guidelines virtually all during the time of the study (2000-2009). A study across different cities in Eastern China also could find no evidence of a “safe threshold”.
Do filter masks do any good?

These cheap, simple respirator masks are a common sight in Beijing. They are so thin that it is easy to imagine that they can’t be doing much of anything, but apparently this simple measure is quite effective. This study from University of São Paulo was based on metabolic response to pollution, and found the response was reduced to undetectable levels by wearing a mask.
Also common in China are indoor air purifiers that continually circulate air through a HEPA filter. The Berkeley Wellness Letter offers some suggestions and emphasizes limitations. A room air purifier provides less effective protection than a mask.

Can B Vitamins Shield you from Harm?
This study looked at short-term effects of particulate pollution only. These include elevated heart rate, suppressed immune function, certain epigenetic changes (DNA methylation), and a decrease in heart rate variability. (The latter is a somewhat mysterious but apparently robust measure of health that has begun to gain recognition as an indicator in recent years [ref].) By all these measures, a modest course of B vitamin supplementation for several weeks preceding exposure completely prevented the physiological response. On the one hand, it’s a very impressive result; on the other hand, what we care most about is long-term damage to the lungs and CV system, and the short-term protection may or may not correspond to long-term protection.
To Exercise or Not to Exercise?
This study finds that the benefits of walking and cycling outweigh the damage done by breathing more polluted air. The claim is that this is overwhelmingly true in moderately polluted Western cities, and remains true in all but the most polluted cities of the developing world. The methodology of the study looks good to me, although the data on which it is based are uncertain. The study doesn’t address high-intensity exercise, which necessarily involves rapid hyperventilation. It is hard to know if lung damage might be caused at an extra-high rate when the body’s cleansing mechanisms are overwhelmed, as they are in cigarette smoking. People in China tend to exercise less on high-pollution days, but when they live in high-pollution cities, they make the most of it and exercise indoors, or outdoors when the pollution is as good as it’s going to get [ref].

The Bottom Line
Mitigating air pollution is an important environmental project, with health benefits that far outweigh the costs. It is indeed a travesty that our EPA is bowing to pressure from GM and Exxon, decade after decade. Mitigation is well worth pursuing in the US, let alone in developing Asian cities. Nevertheless, even in the worst areas of China and India, the air pollution is a major health problem only for a sensitive segment of the population, and overall robs city-dwellers of less than a year off life expectancy.
Two Personal Notes
- I fasted for five days last month, coordinated to end on the Jewish fast day of Yom Kippur. The last two days I took large doses of quercetin, thinking to purge senescent cells. Fasting is supposed to protect normal cells, while sensitizing senescent cells to toxins. Quercetin is a supplement commonly found in health food stores, a flavonoid extracted found in onions and green tea. It has been identified as a senolytic. Results: Difficult to say with any certainty, but I did feel an ease and speed in swimming after I began re-feeding, and perhaps an easing of chronic stiffness in my low back.
- I have a yoga practice that goes back to 1972 and, I believe, has helped me to retain range of motion. The place I feel loss of suppleness most is my lower spine, and MRIs showed a loss of discs beginning 20 years ago. I take daily aspirin, 325 mg at bedtime, and I think I associate this with an easing of flexibility in the low back. Recently, I’ve noticed that if I substitute naproxen (200 mg) for the aspirin, my low back feels less stiff in the morning. Naproxen is a stronger over-the-counter NSAID than aspirin, more likely to produce side effects in sensitive stomachs; some studies claim to detect long-term heart risks. The best reason to prefer aspirin over naproxen is the long history attesting to the safety of aspirin (for most people).
I intend to try more controlled experiments over the next few weeks to see if my first impressions of naproxen’s benefit hold up.
Discover more from Josh Mitteldorf
Subscribe to get the latest posts sent to your email.
Thanks Josh for this post. I was living in Quiappo in the heart of very air polluted Manila in the Philippines for 6 months last year.
After I came home I developed angina and breathlessness and was diagnosed with cardiovascular issues. And I have wondered about the impact of the heavily polluted air of Manila in this development.
Phew, thanks for the reassuring news about reversibility, I had always feared a little that my 5 weeks to Beijing might have more of an effect than just the 3 months of coughing I did afterwards. Some of my friends were actually coughing up black mucus.
I know Bill and my experiences are anecdotal evidence and don’t replace studies, but as we don’t have enough studies to answer everything, we need to take what we can to convince doubters and policy makers.
What pisses me off the most is that gas powered leaf blowers have not been banned, even in California.
These pollute far more than any vehicle ever did and the noise is deadening.
That and wood burning heaters and fireplaces, ban them both and the air would be much better
Amen
If you look at lung cancer incidence, North America is as bad as China (http://globocan.iarc.fr/Pages/fact_sheets_cancer.aspx?cancer=lung). Anyone who has been to China can observe that outdoor air is way worse in China and much higher percentage of Chinese men smoke cigarettes than here in North America. It’s just a personal opinion, but I think we overlook the importance of indoor air. Almost all blue zones are located in islands or peninsula with good air (with the exception of Loma Linda) and warm temperature, people breathe in outdoor air day and night (warm temperature without tightly insulated house and no air conditioning). Even though we have much better outdoor air, but we air condition in the summer, heat in the winter. So we don’t take any advantage of the good air.
In China, lung cancer mortality in the mid 70s was 5.47/100,000, in the early 90s was 17.27/100,000, in 2006 was 30/100,000. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4448492/
So lung cancer definitely has to do with life style/ environmental factors. Statistically, life expectancy is probably still increasing in China despite heavily polluted air, because nobody starves to death no more and infant mortality is practically at zero. But I don’t think air pollution only takes away one year of life. My great grandfather lived to 96, my grandmother lived to 92, but my mother died of lung cancer last year at 82. They all lived in China.
I’m aware of 2 studies regarding the health risks of pollution. The first showed an increased risk of premature death living near a highway. Finklesten MM. Amer J Epidemic. 2004 160:173-177. And Lancet2002 360:1203-1209
Also risk of dementia in Ontario for those who live close to traffic ( less than 50 meters)Lancet 2017. Chen,H
As for naproxen vs aspirin, this has been a long developing story. It was at first thought that the nsaid’s were stronger and safer which is why they all quickly became otc Meds. We have never really been able to demonstrate increased efficacy, however, and they are less safe. As you stated, there is considerable evidence for long term cardiovascular risk for the nsaid’s, but we believed that naproxen was an exception. This was disproved in a recent study by Dr Michelle Bally an epidemiologist at the University of Montreal. They showed that even one week of nsaid’s , including naproxen showed a significant increase risk of heart attacks. Of course it was an association study , but still. Nsaid’s have now been found to potentially lead to a whole variety of problems whereas aspirin, even at 600 mg is safer and as effective as naproxen 200. Furthermore, those who have chronically been on aspirin face an increased risk of heart attack with sudden cessation. Harvard university health 2014.
Paul could you provide a link to the 2014 Harvard research about stopping aspirin leading to a higher risk of CVD ?
I am in that position as I took baby aspiri for 5 years daily but discovered that it caused occult bleeding in the gut and so anemia.
I forgot to mention one other thing that you may find interesting. This rather surprising study was just released:
“25 year physical activity trajectories and development of sub clinical coronary artery disease as measured by coronary artery calcium ” where exercise which exceeded 7.5 hours per week was associated with a very significantly higher risk of coronary calcium scores,avery good measure of coronary artery disease , compared with those who exercised much less. Seen mainly in white males.
There seems to be an exercise sweet spot that is not too little and not too much.
Hi Paul,
Very interesting and surprising finding. First time I heard that exercise can increase calcium deposit in the arteries. By the way, are you aware of any supplement that can prevent calcium deposit in the arteries? Not that I am exercising more than 7.5 hours per week but just thinking that this is something that eventually happen to everyone.
Hi Aldebaran
There is very good evidence that magnesium, vitamin k 2 and IP 6 are all good for that purpose. Doses are 500mg, 200mcg, and 1000mg respectively
I also follow my coronary calcium scores periodically.
Hi Paul,
Thanks for the tip! Just checked IP-6 on webmed. Seems pretty safe for people without clotting disorder or iron/calcium deficient. They mention possible anti-cancer effects as advocated by Abulkalam M. Shamsuddin (who you have already mentioned). Will give it a try.
Calcium deposits don’t happen to “everyone”. I’ve viewed tens of thousands of geriatric CT scans. Several percent are completely clear.
Hi Bill,
Is you saying you is radiologist who reads CT scans or is you “cell culture guy” ?
Hi Paul,
Increased exercise associated with less cardiovascular death and disease in very large number studies. So I guess what study shows is coronary calcium not a very good test.
Huge problem with surrogate tests for disease as opposed to actual disease and death.
How about listing a study in which increased exercise associated with increased death from cardiovascular disease.
Hi Alan,
Great post on coronary calcium (CAC), you really nailed that one. Here is paper: “coronary artery calcium rises with intense exercise.” Here is the catch:
Most of the plaques in male athletes 72% were calcified. “By contrast, most of the plaques in controls had a mixed morphology (61.5%) thus indicating higher risk for rupture.
In second study, 38% in most active group had calcified plaque, compared to 16% in least active group.
The conclusion, “The key point is that while some high volume habitual exercisers have high coronary calcium scores, they appear to have more stable plaque. Stable plaque plus larger coronaries that dilate more in high volume exercisers should be HIGHLY PROTECTIVE AGAINST CORONARY EVENTS.”
Bottom line: calcified plaque is stable, non calcified plaque is more unstable. Unstable plaque is what kills you.
This is reason why need to look at things like coronary events and death from CVD.
They also write:
“It is important to acknowledge the COMPLETE absence of clinical outcomes data in athletes with CAC”. “Although CAC in less active populations has been linked to adverse outcomes.”
What these two studies demonstrated was that high level exercise is good; but CAC scores can be misleading if failure to consider whether stable calcified plaque or dangerous unstable plaque.
It also shows my original point that clinical events like heart attack and death much better than surrogate markers like CAC.
Hi Alan,
Great point! Artery calcification is more complicated than what I was thinking.
Hi Aldebaran,
Should read paper cited, “Coronary artery calcification rises with intensive exercise”.
What is complicated is plaque and the understanding about difference between stable and unstable plaque. Rapamycin by lowering mTOR very effective in stabilize plaque and this why expected to prevent rupture plaque and myocardial infarction. High level exercise helps reduce mTOR and stabilze plaque or prevent destabilize plaque. That is what this study is showing, calcified plaque is stable plaque. So I think this study indirectly confirms possible benefits lowering mTOR.
Hi Alan
We both agree on the value of exercise. I prefer more of a high intensity interval approach and I think that the data is fairly strong.
About CAC scores, I agree that no risk factor assessment method is perfect, but recent studies show a 90% chance of not having an MI over a 12 year period if the score is zero. Much higher than any other risk factor’s predictive ability. If the score is 300 your 12 year risk approaches 50%.
But we are agreeing more than not here
Hi Alan,
I read the paper you have mentioned and completely agree with your conclusion. Having stable plaques lower risk of cardiac events.
Having said that, I am thinking that there might be some value in trying to reduce CAC independently of exercise (which is good for health and longevity). Paul mentioned a very low probability of having MI event with a CAC score of zero. Another reason is that CAC is associated with dementia in the following study (which unfortunately is not open access).
I agree about the limitation of using surrogate markers and it could be that such studies are misleading.
“Coronary Artery Calcium and Risk of Dementia in MESA (Multi-Ethnic Study of Atherosclerosis)”
“Conclusions—Higher baseline CAC was significantly associated with increased risk of dementia independent of vascular risk factor, APOE-ε4, and incident stroke. This is consistent with a hypothesis that vascular injuries play a role in the development of dementia.”
Hi Aldebaran,
As regards Alzheimer’s disease.
AD is microvascular disease as first step and vascular disease starts 20 years before dementia.
ApoE4 carriers great risk and 8 year earlier onset. ApoE4 accelerates microvascular disease.
Microvascular disease and large disease both bad but very different conditions.
As regards zero CAC score, good luck.
Hi Aldebaran,
As general point, biggest mistake in logical analysis is mistaking correlation with actual causation.
Most often there is common underlying factor for both and not real causation
My bet is those doing more PA ate more, and in particular ate more carbs. Studies should be measuring insulin response (see Kraft insulin assays) and so should MDs!
Cheers,
Nick.
I agree about the exercise “sweet spot.”
There are studies that show that marathon participants have a suppressed immune systems for up to 48 hours following the strenuous activity.
I participated in a marathon once. For a few days afterward I felt very ill….weak and depleted in a way that other forms of exercise did not make me feel.
I was hydrated and receiving adequate nutrition, too. Typically I felt great after exercise, but not after the marathon.
I was well trained, and also worked as a freelance fitness instructor, prior to the marathon. Still, the strenuous marathon strained my system.
I never participated in another marathon because I thought that feeling the way I felt could not be a good thing.
Years later I saw a study mentioning the depressed immune system issued, regarding marathon participants.
Then too, there is exercise induced asthma sometimes triggered by strenuous activity, indoors or outdoors, in some people.
Hi Heather,
When people think about what is right level of physical activity, I suggest transport yourself back in time 10,000 years. Then think what seems like right level physical activity. Geronimo said his Apaches could cover 70 miles a day on foot. How does current recommendation of 30 minted 5 times a week compare to what humans use to be.
Hi Alan:
Yes. I have read about the Apache spirit runners….The trance like state, the six minute miles to avoid capture
Still, I do not know if we can draw a conclusion from the Apache that engaging regularly in strenuous 60-70 mile runs has an anti-aging benefit, or is healthy in the long term, because their environment, lifestyle and culture were so different.
The average life span of an Apache in the late 1800s was 35 with 50 being ancient.
Too many uncontrolled variables. No long term observations.
There are researchers who have long believed that too much exercise has diminishing returns.
My point is we live in extreme sedentary society. This sedentary life style plays major role in diabetes and most age related disease.
The sedentary life style is very much promoted by junk science attacking active people.
The reality is old people who cycle 1000 miles a month are very healthy, old marathon runners are very healthy.
Japanese study showed marked benefit walking 2 plus hours a day in 65-75 age group without major illness.
Alan:
I think we both agree, exercise is a good thing. We just disagree on how much and how intense.
Here is a recent Danish study showing that slow and steady pace joggers outlive intense marathon runners:
———————-
http://www.onlinejacc.org/content/65/5/411
From the link:
(( Conclusions The findings suggest a U-shaped association between all-cause mortality and dose of jogging as calibrated by pace, quantity, and frequency of jogging. Light and moderate joggers have lower mortality than sedentary nonjoggers, whereas strenuous joggers have a mortality rate not statistically different from that of the sedentary group. ))
And more from the link:
The Copenhagen City Heart Study (14,15) reported that the relative intensity of walking and cycling and not the duration was of most importance in relation to all-cause and CHD mortality. Subsequently, the Copenhagen City Heart Study showed that the increase in survival among joggers was 6.2 years in men and 5.6 years in women. This particular analysis was performed in a random sample of 1,878 joggers who were followed for up to 35 years and compared with 16,827 nonjoggers. Jogging up to 2.5 h per week at a slow or average pace and a frequency of ≤3 times per week was associated with the lowest mortality. Those who jogged >4 h per week, at a fast pace, and >3 times per week appeared to lose many of the longevity benefits noted with less strenuous doses of jogging (16). This finding was somewhat surprising. )
———–
Alan:
I agree that moderately paced or a moderate pace interspersed with short intense interval bursts is a good thing.
For many years I worked as a fitness instructor in addition to my day job. I no longer have the time for that.
Still, It was very difficult to motivate most people to walk 2 plus hours a day or cycle 1000 miles per month. Some do not have the time, others do not have the motivation.
I mainly encouraged those people to at least work out 20 minutes 5 times a week.
For some very unmotivated people I would be happy if they would do 4 minutes with 20 second intense interval bursts, 5 days per week.
Some exercise is better than none. IMO.
Hi Heather,
The Copenhagen study you posted is the most importance study I have ever seen on physical activity. Studying that paper has caused me to completely rethink and dramatically change my idea on physical activity. This is very excellent paper as end point is death. There is no debate about medical significance of death. Also there is excellent breakdown of speed of jogging (from 12 minute mile to 7 minute mile) and time. This is the definitive work on jogging from perspective of health benefits as regards longevity.
However, jogging is very different from walking or slow bike riding.
I would characterize walking at @ 2.8-3 mph as light physical activity and cycling @ 7 mph as also light. I would characterize slow jogging at 12 minute mile as moderate. [as an example at age 40 I was a 10 minute mile marathon runner; but now 5 minutes of jogging at any speed makes me tired; but I can walk or cycle 2-4 hours/day with no problem (age 74).
So jogging much more strenuous than walking or slow cycling. Note that slow cycling allows going from 7 mph to 12 mph at will.
In an excellent Japanese prospective study 65-75 y/o men had maximum benefit at walking > 2 hours a day (those with serious disease did well walking 1-2 hours a day; but major decline over 2 hours.
The important point is any discussion of physical activity has to differentiate between walking, cycling slow, cycling fast and jogging at different speeds.
As regards 150 minutes a week physical activity; I couldn’t even walk my dogs in 150 minutes a week as we spend 45 minutes every day walking on trails in park. However, the Copenhagen study show that 60-160 minutes of jogging is best amount of time.
As regards mechanism of benefit and injury, my opinion is walking and cycling and jogging decreases insulin resistance in legs.
However, prolonged jogging or running may cause direct injury to heart muscle among other things.
Bottom line, walking, cycling, jogging are all forms of physical activity; but they should never be lumped together as more different than similar.
So agree jogging has J shaped curve. As regards walking and slow cycling, I think people could walk or slow cycle from sunrise to sun set if they wanted to without any negative effect.
Thanks for posting really great paper (Dose of Jogging and long-term Mortality, Copenhagen City Heart Study)
Hi Allan:
I think we are in agreement here.
As you stated: physical activity has to differentiate between walking, cycling slow, cycling fast and jogging at different speeds.
I also agree that a person could likely bike or walk at a light pace all day without harm.
LIMITED joint friendly jogging and running, if a person finds it enjoyable and wears the proper shoes and uses a proper technique is likely good too.
http://womensrunninguk.co.uk/health/running-bad-joints/
From the article:
[ A 2014 study conducted by Dr Grace Hsiao-Wei Lo, Assistant Professor of Medicine at Baylor College of Medicine, found that running at any stage of life doesn’t increase a person’s risk of osteoarthritis of the knee. In fact, it may even help to ward off the condition.
More:
Some loading of the joints is actually good for us. “Running can improve our joint and bone health, especially if we manage the volume and frequency of our runs,” says physiotherapist Stuart Mailer from Kensington Physio & Sports Medicine (kenphysio.com).
“When we run, there is a high stress and load going through our joints and bone tissue that can improve bone density, helping to prevent osteoporosis and osteoarthritis. The bone remodels itself frequently and adapts to the stress it is put through. Running can help our joint health so long as we are sensible with regards to volume and intensity.” ]
I think there is something to be said for either a slow steady exercise for a long time, or the shock of high intense exercise. I’m more of a high intensity sort of guy, as my exercise regime evolved out of a past martial arts practice and it suits my temperament and lack of spare time. But I don’t think there is enough evidence to say one is better than the other at this time.
One thing I would say though. All the fittest, strongest or most impressive athletes I ever met were people who trained all the time. And by that I mean they were almost never not training. Even in the office they would be doing little things all the time to build some attribute. There was a martial artist I knew who has the most ridiculous grip strength. And he got it by just gripping things, all the time and squeezing! He had hands like crabs. Anyway, just a random thought that you don’t have to divide your time up into exercise and non exercise time!
Hi Mark:
I do not have a definitive answer regarding how much exercises is optimum.
Like much of science the information is sometimes contradictory.
Perhaps each person’s mileage varies.
Here is an interesting article:
https://www.nytimes.com/201
7/04/12/well/move/an-hour-of-running-may-add-seven-hours-to-your-life.html
From the article:
“Improvements in life expectancy generally plateaued at about four hours of running per week, Dr. Lee says. … Of course, the findings in this new review are associational, meaning that they prove that people who run tend also to be people who live longer, but not that running directly causes the increases in longevity.Apr 12, 2017”
I expect you are right Heather and each person’s optimal amount of exercise is slightly different, probably depending on how able to respond their endogenous anti oxidant system is. I would expect the level would not be a constant either, necessitating taking it easy on some days and training harder on others. Basically exercise is hormetic and there will be a level that is harmful in terms of longevity. I expect it would be very difficult to exercise so much (or so intensely) that you did more damage than being sedentary, however!
Hi Mark,
When it comes to physical activity, what part of insulin sensitivity, leg muscles and GLUT 4 transporters did you not understand.
Looking at discussion of exercise and physical activity appears terms so broad and include so much totally different activities as to be void for vagueness. Huge problem to lump together totally different things and try to have meaningful discussion. One person talking about 2 hours of cycling and somebody else talking about squeezing ball for 30 seconds not talking same thing.
I don’t think we are in disagreement Alan. I just think a short burst of intense exercise can probably do just as much for insulin sensitivity as a long period of more moderate effort. I believe this effect is mediated by the body’s reaction to a huge, short term effort, which continues for many hours after the exercise period is over. This is my preferred activity because I am (relatively) young, but time poor.
I quite understand that in your case cycling makes much more sense, but I expect the underlying benefits come from the same changes happening in the body.
As I’ve said before, the grip training was just an example, agreed we need to include leg/whole body exercises to make the most of the glucose consuming ability of such large muscles. I expect much of the current obesity crisis is due to people sitting still at office desk for too long and not using their legs at all.
Hi Mark,
I suggest divide physical activity in 3 group:
1. Resistance to increase strength size muscle.
2. Cardiovascular includes HIIT and all activities.
3. Leg muscles burning glucose for insulin sensitivity. This is activity I suggest requires the equivalent in burning calories to 500 calories, which is walking 5 miles. Cycling, jogging would do same thing in less time.
HIIT requires little time for maximum benefit.
Hi Bill
Just to be clear, these studies in no way demonstrate that aspirin prevents heart attacks, in fact it may not This represents more of a rebound effect from stopping it. The first : BMJ 2011;343d4094 ” Discontinuation of low dose aspirin and risk of myocardial infarction”
Also more recently: Circulation: Sept 26,2017,Vol136, Number13
” Low dose aspirin discontinuation and risk of cardiovascular events”
I actually prefer now the safer and probably more effective combination of pine bark 200 mg with gotu cola as well as inhibition of pcsk-9 by fasting.
Thanks for the reply Paul. I wlll look it up.
I was not taking aspirin for it’s negligible impact on heart disease.
I was taking aspirin as research has shown that it reduces the colon cancer. ( Sorry no links on this. But the research i read dates from 2010 in New Scientist magazine.
And yes I am taking Gotu kola and pine bark supplements as recommended by Life Extension magazine earlier this year.
Hi Paul,
More on CAC.
We both certainly agree that best to have no atheroclerosis and have zero CAC score. However by age 70 more than 90% have positive CAC score.
Check out following article: “Study demonstrates need to change scoring system for heart disease”, “Dense heart plaques may have protective quality”. UC San Diego news, 2014.
“coronary artery density (CAC) may be protective against cardiovascular events”.
“Great CAC density of calcified plaques in the coronary arteries was INVERSELY and significantly associated with risk of coronary heart disease and cardiovascular disease (CVD) events.”
“Current scoring systems assume that denser heart plaque (CAC) is more hazardous, but we found the opposite.” “It’s not good to have CAC, but it is less hazardous if it’s more dense.”
This relates to critical issue of stable and unstable plaque.
Getting back to original post about athletes,
This show the athletes (high intensity physical activity) were not able to prevent having atherosclerotic lesions; but they made their lesion less dangerous, even through had denser calcification and higher CAC score.
So your original post about athletes and CAC scores leads to better understanding of CAC scores and significance of dense calcification
I would agree that it’s better if you must have plaque in your coronary arteries to have it “hard” and stable , rather than “soft” and rupture. But my goal is to maintain my score at zero while keeping calcium where it belongs- in bone. Because if calcium has gone awry and deposited in your vessels, it has not done so preferentially, and has possibly also gone to common sites of calcium induced damage such as the aortic valve leading to aortic stenosis, or the breast and prostate giving an increased cancer risk.
If I do get plaque I would prefer a non-calcific stabilization process such as that offered by gotu kola.
As a side note, it is also interesting to me that women who are intense athletes do not get an elevated CAC. This could be, though I’m guessing here, that women tend to engage in more interval-like training exercises like tennis, yoga, dance , etc. , whereas men are more likely to choose treadmills and stationary bikes which are 80% max heart rate types of steady exercises.It also corresponds to the UK study where longevity was mostly associated with racquet sports and not running. But I could be totally off base here.
Hi Paul, Hi Everybody, found most important study on physical activity in men age 65-75. Note this is first rate prospective study done in Japan.
Involves walking and all cause mortality in two groups, those without major critical disease and those with major critical disease (heart disease, stroke, cancer).
Without major disease, walking less than 0.5 hours, 0.5-1 hour, 1-2 hour, equal or more 2 hours. HR: 1.0, 1.03, 0.94, 0.49.
0.49 is equal or more 2 hours. Note no benefit unless walked 2 hours daily.
In those with major critical disease, HR 0.29 if walked 1-2 hours daily, only 0.82 if walked more than 2 hours.
Why this is so extraordinary is in US cut-off is 30 minutes daily.
Here no benefit unless walked 2 hours or more for 65-75 y/o men without critical disease; but those with critical disease had excellent benefit HR 0.29 with moderate activity 1-2 hours/day.
This study shows excellent benefit all cause mortality with moderate activity of walking. Note that this is Japanese study done in major Japanese city. Japanese can walk for more than 2 hours a day. For Americans, experts think 30 minutes is best Americans can do and this study shows minimal benefit for 30 minutes.
Open access entire paper:
Zhao, 2014, “Health benefits of daily walking on mortality among younger-elderly men with or without major critical disease in the new integrate suburban seniority investigation project: A prospective cohort study.”
In my practice I recommend 2 hour a day of walking or cycling. I prefer cycling as more fun, less impact joints and more vigorous.
This is first paper I have ever found that studied moderate activity like walking or cycling more than 2 hours daily. For people into physical activity, 2 hours a day is a typical ; but totally ignored by American experts on exercise.
Hi Alan
As someone who hasn’t missed a week of exercise in his entire life, I’m not really disagreeing. But you must admit that it is certainly difficult to get patients to adhere to a 2 hour per day exercise regimen. I wouldn’t be able to get one patient out of 100 to do it for a whole variety of reasons.
But I am able to get some of them to do 20 minutes of HIIT 3 days a week, and there is ample evidence to support the benefits.
I remember a lecture at McMaster’s University in Canada where they demonstrated a doubling of cellular mitochondrial content using electron microscopy from such an exercise regimen over a several month period. That picture was worth a thousand studies.
Hi Paul,
Agree with correctness of your comment.
However, I see dozen or more people every day cycling or walking 2 hours every day. I see them on same path I’m on while cycling. Many thousands of older persons cycle or walk 2 hours plus a day.
What I was looking for is high quality study of benefits of 2 hours plus cycling or walking.
Very good this Japanese provided good data. First study have seen of prospective study walking 2 plus hours a day.
Since I tell everyone need 2 hours cycling/walking a day; nice to get some medical validation for that advice.
Agreed
Very interesting study. I would love to have two hours each day to do physical exercise (in particular moderate exercise such as walking under the sun, which is a real pleasure). Unfortunately, it will be very difficult to find the time before I retire, I am afraid.
———-
Note from Josh: There is good reason to think more intense exercise works with shorter duration.
Get in the habit of getting up from your desk for a minute every hour.
Work with weights at the limit where your muscles fail after less than ten reps.
Build exercise into your day.
Try Dr Sears’s 12-minute PACE program.
– JJM
Hi Josh,
Thanks for the information about the practice of intense exercises with short duration at work. This sound like a very good plan for active people without much extra time. I’ll definitely try it.
Hi Josh,
In one of your older posts regarding Quercetin you mentioned taking 2.5g on the last evening of your fast and the same dose next morning.
Did you increase the dose this time?
Thanks,
Stephan
Here is a current study published in Lancet on deaths from air and water pollution. It also list a link for a map of the world showing best to worst.
http://www.thelancet.com/commissions/pollution-and-health
All,
Regarding the conversations above wrt atherosclerotic plaques and the benefits of having the atherosclerosis ‘hard/stable’ vs. soft/labile. This of course makes sense but as Dr. Rivas is pointing out, not having it there in the first place would be ‘ideal’. By the way, Dr. Rivas I am also quite enamored with the proven effects of vitamin K to get calcium out of circulation and back into the bones.
I wanted to point out something not discussed yet. I am going to ‘throw this out there’ and am not a researcher nor a medical professional (a professional engineer). I have been extremely impressed (or duped) by talk regarding one of the vitamin E’s in particular gamma tocotrienol in potentially eliminating and even regressing atherosclerotic plaques (as measured in the carotid arteries).
I will reference you to this interview by Dr.Passwater with a couple of researchers and therein you will also find references to the studies. (This is also highly promoted and marketed by Life Extension Foundation and others).
I would sincerely appreciate any discussion on this.
Until now at least I’ve added a ‘complete vitamin E’ to my regimen with all 4 tocopherols and 4 tocotrienols in an effort to eliminate the soft/labile atheroscleortic plaque in addition to vitamin k2 intake and plenty of greens (for K1).
Hi Clinton,
Personally, I would be careful supplementing fat soluble vitamins (A, D, E, K). Since fat soluble vitamins are stored in your body for a long time, they could pose risk of toxicity in excess. http://extension.colostate.edu/topic-areas/nutrition-food-safety-health/fat-soluble-vitamins-a-d-e-and-k-9-315/. I would try to find them from fsood sources. Rice bran oil can be bought online as a source for tocotrienols.
I have consistently recommended higher levels of vitamin D than we can reasonably get from foods. There is good statistical evidence for people with the highest levels of vit D having the lowest risk of cancer, and toxicity is not an issue up to blood levels exceeding 100, which is hard to achieve even with 10,000 iu per day.
– JJM
Yes, sorry I forgot to mention Vitamin D is the exception to the rule of the fat soluble Vitamins. Vitamin E is the most worrisome here.
Thank you Cassia, Josh and Paul,
I would rather ‘do no harm’ than take too much of something that might accumulate. Any comments on ubiquinol (non-reduced CoQ10) as a way to mitigate oxidation of LDL and maybe NOT accumulate?
Thanks all,
Clinton
Hi Clinton
Harm is always a dose-related phenomenon. Tocotrienols have been studied now since 2008 and multiple studies have shown no harm when they are free of tocopherols, such as those derived from Annatto, and when the dose is 50-125mg’s. Dr. Tan and others wrote a 400 page textbook on this in 2012 detailing the many studies for both effect and safety. There is substantial evidence for the prevention of the big 2 age-related diseases, CVD and cancer, so in my mind the enormous benefits outweigh the risks ( if any). Ditto for 200 mcg of vit K2.
Here is the interview by Dr.Passwater regarding tocotrienols and atherosclerotic plaque regression:
http://www.drpasswater.com/nutrition_library/tan_1.html
Thanks and Regards,
Clinton
Clinton
That was an excellent interview with Dr. Tan on tocotrienols and quite a coincidence since I had just read a study on how potent they are against several cancer lines, and also the synergy with curcumin in a fat emulsion. Int J Mol Sci 2016 Nov 17 (11) 1792. Akshay will attest that I just asked his advice on which fat emulsion would work best.
I had actually only heard of tocopherols and was not aware of how potently and safely tocotrienols lower lipids, so I thank you for this since rapamycin can raise lipids somewhat and I like to avoid statins due to side effects.
I’m also a big fan of vitamin k2 and mg+ to keep stave off metastatic calcium deposition and I’m grateful to life extension for making me aware of this issue. IP6 gives yet more protection .
It would be impossible to get an adequate effect from food sources.
Thanks Josh for another great blog post. I wonder with air pollution. Where is the limit of hormesis here? There must be some amount of pollution that is beneficial, because the body can fight back against such things, though granted this will be different for different people. I’m not saying we shouldn’t strive for cleaner air, but there may be a point at which reducing levels further is not beneficial.
Hi Mark,
Hormesis and toxins is great. I don’t smoke myself, but I try to hang out in smoke filled rooms, just to get the benefit of second hand smoke for hormesis. I also take a toxic chemical supplement daily with arsenic, cadmium, lead, mercury and bunch of petroleum related compounds. Big hormesis fan.
Very droll Alan.
But what about radiation hormesis, then?
‘Effects of Cobalt-60 Exposure on Health of Taiwan Residents Suggest New Approach Needed in Radiation Protection’
Chen et al., 2007, in Dose Response.
Hi Mark,
Big up to you.
One very remarkable paper..
Very funny Alan!
The tricky part is to figure out how to get the right dose of toxins since food vendors do not typically document how much cadmium and mercury are in their products. I am concerned that since I have switched to the “Endangered species” brand, my chocolate does not have enough cadmium.
Regarding radiations, it seems that the scientific community is divided on the idea that low radiation exposure is beneficial. The Taiwan study mentioned by Mark have created some controversies.
“Estimates of Relative Risks for Cancers in a Population after Prolonged Low-Dose-Rate Radiation Exposure: A Follow-up Assessment from 1983 to 2005”. Radiation Research
On the other hand, it seems that hormesis related to sun exposure is less controversial. From wikipedia:
“In an Australian study which analyzed the association between solar UV exposure and DNA damage, the results indicated that although the frequency of cells with chromosome breakage increased with increasing sun exposure, the misrepair of DNA strand breaks decreased as sun exposure was heightened.”
This is the study in question:
“Sunlight and vitamin D affect DNA damage, cell division and cell death in human lymphocytes: A cross-sectional study in South Australia”. Mutagenesis. 27 (5): 609–14
Aldabaren, I live in South Australia close to Adelaide..I do not like to dump on research done here in Oz but I am a bit dubious about this study and it’s conclusions.
There has been a sustained publicity campaign to get all people to “slip, slap, slop” ( slip on a shirt, slap on a hat and slop on sunblock ) since the early 1980’s and the discovery of the Ozone hole..It’s been a very sustained publically funded national campaign in the media and doctors surgeries, pharmacies, kindergartens childcare centers & schools.
An illustration : .Children at primary schools here are forbidden going outside during playtime & lunch breaks, in Summer if they do not wear a hat !
Actually going out in the sun in Summer is now popularly seen as a risky behaviour..
So I wonder about the extent to which the participants of this research trial actually spent time in the sun.
My doubts are increased by the simple fact that this was an observational study with participants being asked to recall in a questionaire how much sun they had been exposed to in the previous 6 weeks..
Bugger ! I can’t remember how much sun I was exposed to yesterday.
A final note ; sales of Vitamin D capsules have soared in the last decade as the general population here have become aware of the need for vitamin D when not getting sun exposure. They are now a major supplement sold in pharmacies and supermarkets..
Hi Bill,
To be honest, I was just mentioning this study as an example of hormesis from sun exposure as quoted by the following wikipedia: https://en.wikipedia.org/wiki/Radiation_hormesis
Although this study is not directly about hormesis, they have observed an hormetic effect related to low dose sun exposure:
“Therefore, the reduction in BN-NPB with increased UV dose that we observed seems counter-intuitive unless, perhaps, exposure to low dose UV in some way protects against DNA strand break misrepair or telomere end-fusions, from which BN-NPB are also thought to originate, although without generation of accompanying MN (14,23).”
I agree with you that one of the limitations of this study is their subjective way to measure sun exposure by questionnaire.
“Participants’ solar UV exposure in each of the 16 weeks before blood collection was calculated from their recalled hours of exposure and the average ambient UV irradiance between 9 am and 5 pm at their location in that week. ”
Thanks for catching that!
I think hormesis is a good stress buster, I.e. don’t worry overly about small amounts of toxins or radiation, etc, as your body may well end up stronger for it, providing you don’t end up chronically exposed, or acutely exposed to too great a dose.
Hi Aldebaran,
If hornesis working would have U shaped curve.
A very small level could stimulate a protective response. A larger dose would still be toxic.
However, idea that any radiation protective gives excellent support to Hormesis theory.
Hi Alan,
The U shaped curve is a very good way to describe hormesis. And it looks like hormesis is working in even more circumstances that I would have thought. For example, low doses of amyloid aggregates:
“Strikingly, the exposure to non-harmful low doses of amyloid aggregates exerts a protective stimulus in models of Alzheimer’s and Parkinson’s disease”
Extracted from:
“When less is more: hormesis against stress and disease”:
Since we are discussing about atherosclerotic plaques, I thought it might be worth mentioning that a technology based on ultrasound is being investigated for plaque removal. I don’t know if this technology will succeed or not and in which time-frame but it looks interesting.
J Ultrasound. 2015:
“Removing atherosclerotic plaque created using high cholesterol diet in rabbit using ultrasound”
And also:
J Ultrasound. 2016 Jan 12
Feasibility study for removing calcified material using a planar rectangular ultrasound transducer.
This is odd. This study in msphere 2017 2 (5) by Gaorui Bian.
In a collaboration between Canada and China they looked at 1000 people between the ages of 3 to 100, focusing on the 90 to 100 year olds whom they termed “ridiculously healthy” and free of any past history of illness, and the thing that they found was that all of them had the identical gut flora of healthy 30 year olds. They of course aren’t sure if this is just a health marker or if it’s some sort of cause and effect.
It will be interesting to see where this goes but it’s becoming increasingly clear that gut flora is very important to our health.
Hi Paul,
Very interesting,
Gut flora can make all sorts of chemicals and determine what enters blood stream.
So makes complete sense that right flora could be very helpful.
Nice find
Hi Alan
Just not at all certain how to keep my gut flora the same as a 30 year old, or even how you would evaluate that.
Did you see this one Alan?
“Chronic repression of mTOR 2 ….gut flora” Mi-Ja Jung Scientific Reports 29 July 2016
Showing that chronic rapa screws up the gut flora. My question to you is, why do they keep studying doses and frequencies of rapamycin that are Not recommended for anti-aging in humans? Blagosklonny has made this perfectly clear!
It’s almost like they have an agenda. Enough already.
Sorry for the rant.
Hi Paul,
Million people have used Rapa for transplants and only handful for anti-aging. So us handful need to figure out best dose best interval etc.
As regards flora; don’t need 30 y/o: we need somebody 105; they have good shit.
LOL
That’s true
Well we know rapamycin treatment in mice changes their microbiome for the better. I’ve read that in several papers.
Good to know
The gut is obviously a very important barrier stopping lots of nasties getting into the blood, and once it starts to leak will massively ramp up inflammation. So I would expect gut health to be a necessity to reach old age Inna good state. It would be interesting to find out how causal this is. I have always thought telomere length to be important here as stomach lining turnover is fast and inflammation likely to impede replacement.
Hey Mark
I think that you’re right in regards to fitness, but in terms of mortality rates, I think that exercise follows the law of diminishing returns. Just getting someone out of a hospital bed to walking around the yard carries a great benefit, ditto for the transition from totally sedentary to mild to moderate exercise levels, but I think then going that extra step to intense exercise of hours a day offers a relatively modest extra return on the time investment. After all you may then spend 3 to 5 years of your total lifetime exercising for a net return of the same number of years give or take. Also you could have been spending that time doing something else– also worthwhile. As an avid exerciser, I often consider these things.
Paul:
I agree.
Bigger muscles or stronger grip strength or being more buff than one’s peers may not necessarily equate to a longer life span.
It may not even always equate to feeling healthier, depending on the circumstance.
I was only using grip strength as an example. My point was you can build exercise into your routine without it having to take a huge amount of time.
Hi Mark:
I agree, and I find your posts and all the posts here very informative.
I think perhaps to my mind exercise is different than physical activity. Semantics, perhaps?
Alan in another post pointed out that someone could ride a bicycle all day, perhaps as a leisurely, mildly paced form of transportation, without the harm or oxidative stress that some researchers believe is caused by extreme sustained endurance marathons in which a person is going full out for a long period of time, in order to win the event.
To my mind riding a bicycle or walking at a leisurely or light pace is not really exercise, it is simply movement.
Movement is still good. …..moving more and eating less is always a good thing, to my mind. Unless their is a medical reason to do otherwise.
Alan is right, too, most people not only fail to exercise, they fail to move their bodies enough, preferring to depend cars or public transportation to get from one place to another, even in a city with abundant sidewalks or biking paths.
To my mind, exercise is an activity requiring physical effort, carried out specifically to sustain or improve health and fitness.
Simply walking or biking from one place to another is not exercise but physical of activity of any sort is better than sitting in a chair all day.
Physical activity is all about mTOR. Physical exercise is about insulin sensitivity. Insulin sensitivity is all about leg muscles need for glucose. All about GLUT4 transporters. So walking or cycling increases activity GLUT 4 transporters, increases insulin sensitivity decreases insulin level and decreases mTOR.
Also 75 y/o age group only have ability to cycle moderate speed or walk @ 3 mph.
I do physical activity over 2 hours a day at highest level right for me. This summer cycled 1000 miles each month.
Additional comment for Heather regarding physical activity and insulin sensitivity.
I take weekly Rapamycin. This reduces output insulin. But I don’t want increase glucose and non-enzymatic glycation. So increase demand glucose leg muscles and increase activity GLUT4 transporters. Nobody tells the GLUT4 transporters how fast I cycle. All they know is leg muscles need more glucose, hence glucose sensitivity which is goal.
Hi Alan:
All that you cited in all your posts, is accurate, however, there is still no proof that EXTREME physical activity will extend life span and there is more proof as in that extreme exercise can cause harm.
I did not say that exercise was a negative in general when done in moderation. I was talking about marathons.
Also, regarding your support for rapamycin, which I am taking along with LDN, I would find it helpful for you to disclose your business interest in promoting rapamycin. Do you profit from patients who take it?
Hi Heather
I like your combination approach and I do the same. You’re hitting multiple aging pathways as well as preventing multiple age related diseases. For additional synergy you should consider reading IP6 by Shamsuddin. It also prevents all age related diseases to a large extent and again through a different and unique pathway, also very safe.
Tocotrienols are now also very much on my radar for very similar reasons. See Dr. Barry Tan and his excellent book on the subject.
Hi Paul:
Thank you for the kind suggestions.
I did see your other post regarding Dr. Shamsuddin. I read his research and ordered Cell Forte.
I take it at night after not eating for about three hours and I can say it really induced a sound refreshing sleep.
I had been taking about 100 mgs of inositol as part of the B-complex but not the inositol hexaphosphate
Thank you for pointing me to Dr. Tan’s book. I will read it.
I do already take tocotrienols. I have been taking it for quite awhile with no negative side effects.
Interesting to see that more and more people are starting LDN + Rapa. Heather, how did you get started and wha,t is your current regimen (dosage, frequency etc.)? …and agree, taking advice from someone without financial interest would be preferred.
Hi Ole
Do you know others on rapamycin?
Hi Ole:
I am healthy so I started at very low dosages of both, not therapeutic dosages.
I wanted to ensure that I did not experience side effects.
I may slowly ramp up the dosages as more research comes in.
I take 1 mg. of Rapamycin (Sirolimus) once per week and 2.25 mgs Low dose Naltrexone twice per week.
I cycle this regimen one month on with 2 weeks off. I have been doing this for about six months.
So far no negative side effects.
I was healthy and energetic to begin with so I can not say that I saw any amazing change, but definitely nothing negative.
My goal is preventive.
With most things that are preventive, the healthier you are the less likely you are to notice any change.
I did not expect to notice a change given that I feel fine. My concern was more about negative reactions in any form.
I was happy to find this blog.
Hi Heather
I’m reading a textbook on tocotrienols by Ronald Watson , a biochemist at NIH , and he shows in enormous detail with hundreds of studies how they protect against CVD and cancer . My only issue is that they also inhibit telomerase activity, but I’m not sure how meaningful it is. Any thoughts?
Paul you would agree inhibition of telomerase activity may not be a good idea.
In the text Watson brings up telomerase inhibition as one of the many pathways that tocotrienols prevent cancer. The data on this is significant and the pathways seem very sound, but in general I would agree with you. It’s possible I suppose that the inhibition in cancer cells has a major positive effect , whereas the degree of telomerase inhibition in somatic cells may be relatively minor and of little consequence. It’s not clear to me. What do you think?
If Watson says this then I would reconsider as he doesn’t conclude without thorough analysis of the molecular ramifications
Hi Paul:
I do not know enough about telomerase too comment in any valid way on what the significance of a reduction when taking tocotrienols would be beneficial or detrimental.
Also I do not know how the Tocotrienols used were extracted.
Were all the Tocotrienols used synergistically …alpha, beta, gamma, delta??????
Perhaps the reduction in telomerase can be offset with other benefits of the tocotrienols remaining, and if increased telomerase is a good thing, it can be increased in other ways, thereby retaining beneficial aspects of tocotrienols while adding factors that increase telemerase.
Also, perhaps the inhibition of telomerase is an adaptogenic factor.
Or. maybe Tocotrienols simply down regulate telomerase in certain situations.
I am sure you are already aware that the studies on telomerase are conflicting. For example mice with elevated levels of telomerase have higher cancer incidence and do not live longer. Telomerase also favors tumorogenisis.
I do know that I have been self-experimenting with Tocotrienols since 2010 without any negative effects revealed subjectively or in blood work ups.
I have no health issues, so I saw no changes in blood work.
Olive oil contains tocotrienols and studies consistently show a benefit to consuming virgin olive oil.
Paul:
I did try TA 65 once, and did not find an subjective benefit or change in blood work with that either, after one year of supplementation
I stopped taking it because it is expensive. I switched back to Astragalus which has the same active Cycloastragenol component of TA 65 in a much smaller dosage. I am hoping for a cumulative effect.
I once read that Astragalus in Traditional Chinese Medicine translates roughly to “old man hair still black”
Here is some other interesting information.
[Various studies have shown that alpha-tocopherol interferes with Tocotrienol benefits. High levels of α-tocopherol increase cholesterol production. α-Tocopherol interference with Tocotrienol absorption was described previously by Ikeda, who showed that α-tococopherol interfered with absorption of α-tocotrienol, but not γ-tocotrienol.[ Finally, α-tocopherol was shown to interfere with Tocotrienols by increasing catabolism.
Many very good points Heather. I think that it is possible to counter the telomerase effect with other supplements. Mark listed a few that he got from Bill Andrews.
Telomerase and telomeres are a confusing and conflicting subject.
This 400 page textbook that I’m plowing through on tocotrienols is crazy complicated but also very convincing. Seems to be able to protect against all age- related diseases, like rapamycin and IP6, but through different mechanisms. Certainly worth taking them, but yes not with alpha tocopherol which does inhibit their effectiveness.
Several studies have come out just recently showing remarkable effectiveness against a whole variety of cancers, including the very hard to cure ovarian.
Fascinating discussion. So many of these going on at the moment. There are a lot of beneficial supplements that appear to inhibit telomerase. I think of these as hormetic substances; they generally challenge the cell in some way, but end up making it stronger.
Berberine has quite a strong affinity for telomeres, and actually can block telomerase from extending the telomere, plus exclude telomerase from the nucleus. This is not always a bad thing, not only for its cancer preventative properties, but also because the telomerase actually acts as a protective substance in the mitochondria, making the cell more stress resistant. And of course Berberine also has direct effects on the mitochondria as we’ve already discussed.
I just used Berberine as an example. There are many similar supplements that are hormetic in some way, for example some even increase ROS, but this stimulates endogenous anti oxidants and ends up over compensating, I.e. glucosamine.
Of course if you are supplementing with the hope of extending telomeres than you wouldn’t want to take anything with the opposite action at the same time. It would depend on how long said substance takes to break down, but I’d try and separate them by 12 hours if possible.
If you think about it, according to E Blackburn things like poor sleep, diet, stress etc. are competing with other things like good sleep, exercise, meditation, etc. to alternately bring telomerase up and down just as a part of normal life events. Seems like a natural course.
I have a real love/ hate relationship with berberine. Many things I love about it, some I don’t, but I understand that you were only using it as an example.
Agreed Paul, Berberine is definitely effective, but has its downsides. Does anyone know if the Life Extension AMPK activator is any good? Seems expensive but has some cracking ingredients.
There seem to be a lot of supplements that are anti cancer and have an obscure or very complicated mechanisms, curcumin, vit E components, IP-6, etc. I reckon what is happening is that these substances are forcing cells into some kind of epigenetic state, where they are having to adapt epigenetically to the presence of these substances. And perhaps that is precluding the epigenetic and mitochondrial changes that are required by cancer. It’s a kind of protective stress. Think it will be a good while before we get a proper, detailed explanation.
Mark
About the AMPK activator from LEF. Some years ago I gave metformin a try but it gave me fatigue so I stopped it . At about the same time I read about some village in Asia where the residents are very long lived and the only thing that distinguished them from the surrounding areas was that they drank this tea regularly called Gynostemma. I did some research on this and found out that lef was selling it, mixed with hesperidin, as an AMPK activator, very similar to metformin. So I tried it out for about 6 months and it probably works because it gave me almost the identical feeling of fatigue that I got from metformin.
I’m not sure why I’m so sensitive to both products. Now I just drink the tea and that seems to be ok.
How did you take the LEF AMPK tablets Paul, with meals? I was wondering if we could do what someone (maybe Aldebaran or yourself) suggested, and take something relatively mild when you eat to moderate the sharp insulin spike which activates MTOR so strongly. In theory that could be more effective than a more general suppression. I’ve been experimenting with vinegary things like pickled onions and it seems to help a little.
Hi Mark
I would take the AMPK in the AM with food.
According to life extension the combination of maqui berry and clove extract prevents most of the after meal glucose and insulin spikes. Might be cheaper to buy it elsewhere.
Hi Paul:
When you took the Metformin did you supplement with the methylcobalamin form of B12?
If not, using B12 may have helped.
Metformin seriously depletes B12 (cobalamin ).
In some B complex supplements they use (cyanocobalamin) and some people, due to several factors, can not metabolize cyanocobalamin to the active form methylcobalamin.
Methylcobalamin, the active form,is absorbed better.
One of the first signs of B12 deficiency is fatigue.
Sublingual methylcobalamin is absorbed even more efficiently than swallowing a capsule.
Hi Heather
Those are great points. I was taking cyanocobalamin because I wasn’t aware of the issue of conversion. I’ll get the sub Q methylcobalamin. That might be the answer. Thanks
Heather I am not sure if your dosage and frequency of LDN is optimal. If you can please read published interviews of Dr. Behari who discovered the benefits of LDN.
Hi Askay:
Thank you for the information. It is much appreciated.
I am familiar with Dr. Behari’s literature.
I am aware that the suggested dose is too low.
I prefer to start low and than ramp up slowly.
Heather this may not be compared to typical dosage deliberations like hormesis it seems LDN delivers the wanted benefits only in a narrow range of 3.5 to 4.5 mg. Although it’s not too expensive but may be a waste unless I am remembering incorrectly. Also Dr. Behari had suggested 3 months to 6 months daily night time pill with a 1 month break in between.
Hi Askay:
If I were treating one of the health issues knownn to be helped by LDN, I would take the dosage suggested by Dr Behari.
Behari’s dosage may well be the optimum dosage.
However, I am healthy and my brain chemistry is well balanced and I do not experience pain or depression.
I am taking LDN as a preventive measure not treatment.
There are other researchers who suggest lower dosages (for some people) due to a build up.
Here is an excerpt from an article by Mark J Donohue discussing LDN with various researchers.
————————————-
Dr. Boyle said:
****” I do adjust the dosages… some patients do need to take a drug break… I think there are patients that aren’t so endorphin deficient and need a break of a day or two every now and again… if somebody is going down is it that they are not taking the drug or is it the case that they’ve got too much… it’s a new idea… consider the possibility that we are over treating consider a bit of a break from the treatment and that might work.” (Dr. Boyle) ****
And more….
Dr. Zagon said:
*****”Also, Naltrexone is cleared by the liver, and an impaired liver function may slow the clearance of the drug from the body.
If this is the case each additional dose might be adding to the load in the body. In such cases dosing should take place every other night or every third night, rather than nightly.
“… one of the things we’re learning is, we were giving low-dose naltrexone and OGF (opioid growth factor) every day.
We’ve got a study right now that shows you can give the opioid growth factor once a week and you can get a better effect than you get every day.
… that’s what research is all about.
That’s going to translate to the fact that people don’t have to take this growth factor everyday… they don’t have to take low-dose naltrexone everyday…
… and we’re also finding out that some people… they’re actually taking too much low-dose naltrexone.
In fact what they will do is they are going to feel that they are having a very positive effect but maybe 6 months to a year down the road they’re going to say I’m losing that effect.
And I’ve already had to help about a dozen people so far about that… they reach me… and it’s not working anymore… what’s happening?
Well the reason why it’s not working is because there building up too much naltrexone so their effects are not going to be as great.
So what was the result of that… they had to take the naltrexone every other day
…and in some cases, some of them are taking it every third day now… and the first thing that comes back is… oh it’s working beautifully again.” (Dr. Zagon)
That’s some great info Heather. I’ll start experimenting with different dose frequencies.
Heather thanks for these quotes apparently further research has emerged post Dr. Behari – I stand corrected. Paul please note. It seems from Heather quoted even once a week can work for the healthy.
It’s a strange drug. Dr. Turel, the neurologist, worked with Zagon for 30 years, and when I spoke to him on the phone he said that once the endorphins are upregulated by ldn the effects can last for 2 months. But yet , he still takes it everyday, but I think maybe less is more.
Hi all:
I forgot to include a link to the article regarding alternate LDN dosing schedules.
When you go to the link scroll down to report #19.
A pdf will open, then scroll down to close to bottom in the section titled “how to take LDN.” That is where various dosing schedules are mentioned.
Here is the link:
http://www.toxipedia.org/display/toxipedia/Mark+J++Donohue
I have just begun taking low dose rampamycin (2mg/week to start). I recently read that exercise raised MTORC1 levels which seems to contradict the belief that exercise, within reason, should be a significant part of any ant-aging program. It would seem that exercise, without Rampamycin would be counter-productive to anti-aging and exercising while taking Rampamycin would have the effect of negating the muscle/strength benefits of exercise. Very confusing.
Lawrence –
Let’s be clear about the basis and firmness of our knowledge. We know for sure that exercise is good for lifespan. A huge number of studies in animals and humans support this benefit, with both direct and indirect evidence. On the other hand, our hypothesis about rapamycin is still tentative. Studies in mice look promising. People who try it report, anecdotally, few problems. So early adopters are optimistic.
Theory in biology is always tentative and qualified. mTOR has many functions, and we can’t conclude anything with certainty.
The bottom line is that exercise is a solid part of any life extension program, and rapa is still in the early phase of experiment.
– Josh
Many thanks for your prompt response. Exercise plus Rapa and other potential anti-aging supplements/pharmaceuticals will continue to be part of my effort to fight the (dis)ease of growing older. (I will turn 71 next month).
The key thing to remember is that rapamycin should be taken intermittently, for example once per week (although no one yet knows the best schedule and dose yet for humans). As Alan somewhat grumpily says, Blagosklonny is the authority on MTOR.
Rapamycin’s biological half life is 57-63 hours, using 60 hr for easy calculation, it would take 4×60 hours = 10 days to eliminate 93.75% (50%+25%+12.5%+6.25%) of rapamycin from your body. To qualify intermittently, I would think one should take it once every 10 or more days. Just a thought.
Thank you Cassia
And to add to that you would have to take it every 12.5 days to get it down 97%. May have to reconsider the dosing intervals, but I wonder if 88%at one week vs. 94or97% matters from a clinical point of view. Maybe it does.
Make it every two weeeks, but maybe at a higher dose? Or even once per month. What we want is a temporary but big hit to MTOR. I’ve experimented with bigger doses and then used curcumin to degrade rapamycin faster. Just something to consider.
Mark
I’m forever contemplating dosing and frequencies for optimal effect. Based on the half life it would seem that every 2 weeks might actually be the best and I could then double the dose as you say.
I keep remembering the mouse study where they were really blasted with rapamycin for something like 3 months and then it was stopped. They did very well with that and had a significant life extension.
Also if you consider the starvation effect on holocaust survivors where TOR inhibition must have been significant, but for a period of about 18 months,and then it was over. Again it was a potent but transient TOR hit, but a significant longevity effect.
A lot to consider.
So doing the math it would seem that with an 88% clearance of rapa after 1 week, then if you’re taking 2mg’s say every week you keep adding on to a certain remaining blood level , so it would work out like this:
Week 1 2mg
Week 2 2.2mg
Week 3 2.46
Week 4 2.75
Week 8 4.32
Week 12 6.72
It really starts to add up. Better to go every 14 days at 4mg and then you’re getting the monthly dose that you actually want without the cumulative effects of the half life. ( unless I did the math wrong)
Hi Paul,
Let me suggest another way to do the math.
Whatever dose you have at the beginning of the week will be divided by a constant factor at the end of the week. So let’s compute this factor.
Each 60 hours the dose is divided by 2.
A week is 24*7 = 168 hours = 2.8*60 so the factor is 2^2.8 = 6.96 so roughly 7. It means that whatever dose you have at the beginning of the week will be divided by 7 at the end.
Let’s assume you take 2 mg every week.
At end of week 1 you have 2/7= 0.28mg
At end of week 2 you have 2.28/7 = 0.32mg
At end of week 3 you have 2.32 / 7 = 0.33mg
At end of week 4 you have 2.33/7 = 0.33mg
So the key is that the maximal dose at beginning of each week converge very quickly to 2*7/6 = 2.33 and never go above.
Thanks a lot for that correction Aldebaran, math was never my strong point . I feel much better now .
But still I’m wondering if weekly dosing is optimal, but maybe it is.
Paul,
The only way I can think of to precisely answer about the optimality of the dose would be to do more human trials. However, I am not sure when this will happen. Maybe Alan has a better suggestion.
One thing is a certainty Aldebaran, l’ve taken all kinds of supplements over the years, as well as a very strict diet and exercise program, and I’ve never noticed anything quite as beneficial as weekly low dose rapamycin.
I especially notice it in my ability to run hills and my rapid recovery time.
I intend to get an echocardiogram to see if it has increased my cardiac ejection fraction which I strongly suspect it has.
You mentioned ARB’s and angiotensin inhibitors. I tried that back in August while hiking through Yellowstone and got every conceivable side effect. Unless you’re hypertensive, they’re not a great idea.
Akshay has mentioned Andrographis several times and it’s multiple benefits. I checked it out some and it’s pretty impressive. Might be worth looking at.
Hi Paul,
If 88% clearance 1 week.
Week 1 2.0
Week 2. 2.27
Week 3. 2.27
Week 4. 2.27
Hi Alan
Thanks.It seems odd to me that you’re not adding more drug to an ever increasing blood level each week in a cumulative sort of way since it’s never 100% cleared.
But then again, as my son who’s a physicist at Hopkins , frequently reminds me, I’m math challenged.
Hi Aldebaran,
Other main consideration is indication. Healthy 40 y/o wants to delay aging one thing and person carrier ApoE4 who needs to prevent very high risk AD very different clinical situation. Also big individual variation sensitivity response etc. However, agree with your math and liked Tartokover comment. Haven’t seen his name in long time.
Hi Paul,
That’s quite an interesting personal experience about rapamycin! In pratice, what blood parameters would you recommend to monitor with low dose rapa (WBC, RBC, FBS, insulin, others?).
I have a couple of other questions. Can I send you an email?
Thanks
Of course
[email protected]
Hi Alan,
Thanks for complementary information about rapamycin. Always useful to get your input.
Mathematically Correct Answer
D = Dose
x = Fraction left after dosing interval = amt at end of interval/amt at start of interval
N = number of sequential doses
M = concentration multiplier after many doses. I show below that M = 1/(1-x)
Peak concentration = (M)(D)
Trough concentration (x)(M)(D)
Proof:
xD = amount at end of 1st interval
D+xD = amount immediately after 2nd dose
D+x(D+xD) = amount immediately after 3rd dose
D(1+x+x^2+ …x^(N-1)) = amount immediately after N th dose
The power series is our multiplier M
It can be compacted by multiplying by x & subtracting as follows
M-xM = 1-x^(N)
M = [1-x^N]/(1-x)
For x 0
M = 1/(1-x) q.e.d.
Example: from half-life calculator
at https://www.miniwebtool.com/half-life-calculator/?n1=&n2=5&n3=168&n4=60
1 Week interval = 168 hrs half-life = 60 hrs, an amount of 1 decays to 0.14359
x=0.14359
M = 1/(1-0.14359) = 1/0.85641 = 1.1677
2mg -> 2.3354 peak 0.3353 trough
This is interesting. Research out of Harvard in Cell Metabolism, Oct 26,2017. Heather Weir
” AMPK and calorie restriction promote homeostasis and plasticity of networks formed by mitochondria. Mitochondrial networks change shape according to energy demand, however, this ability declines with age. Dynamic remodeling of mitochondrial networks by fusion and fission promotes maintenance of cellular homeostasis.
By restricting calories in the diet of roundworms, the researchers found that the worms maintained a youthful fused mitochondrial network shape with age.
The youthful networks lengthen life by communicating with peroxisomes within the cells to alter fat metabolism.
Our work shows how crucial the plasticity of mitochondrial networks is for the benefits of fasting. If we lock mitochondria in one state, we completely block the effects of fasting or CR on longevity.”
This is in agreement with what I’ve said previously about the importance of fission. A well fed state tends to fusion and less quality control, especially as metabolic dysfunction sets in and ATP becomes harder to come by, so mitochondria fuse to get more energy and do even less quality control. We humans really do best in a half starved state!
One thing I hadn’t considered much before is the importance of peroxisomes in this process. Peroxisomes are important because they break down long chain fatty acids, a process hard for mitochondria and also producing a lot of ROS. This is the reason the brain loves glucose, because long lived neurons really need to steer clear of ROS. It sounds like a well fed state can lead to this signalling breaking down with a consequent rise in ROS as mitochondria break down more fats. Very dangerous for those at extra risk of dementia.
I figured that you would appreciate that article, and understand it a hell of a lot more than I could. I’m now wondering if rapamycin is sufficient or should it always be combined with CR/ fasting?
We are using a number of approaches to mimic the full benefits of calorie restriction.
Nicotinamide Ribose tablets (or possibly just as good, taking Nicotinamide and D-Ribose) is a way to force mitophagy (more fission and disposal of poor quality mitos). This approach synergizes well with intense exercise.
AMPK activators don’t do it as directly but they are essentially signaling that energy is scarce, so will be pushing in that direction too. AMPK activators are also downregulating MTOR so reducing cellular hypertrophy and senescence. I think AMPK activators make fasting easier (not sure though).
Finally rapamycin is increasing the efficiency of mitochondria by restricting the protein synthesis of the electron transport chain units to only what is absolutely necessary. And of course Rapamycin is by far the most powerful inhibitor of MTOR we have.
Have we missed anything? It would be more certain to get the full CR benefits seen in lower mammals by doing strict CR. But as we know that is very difficult to stick to and actually want to continue living!
A small part of me hopes we could better the effects of calorie restriction in terms of longevity with our approach. However I think it is more likely we are just finding more tolerable ways of doing it and that all our efforts will likely be a healthspan benefit only, with very little additional life on top of any maximum we could have conceivably reached. Of course that is not nothing, living to 90 or 100 in good health is a worthwhile endeavor.
Hi Mark
As usual your comments are chock full of insightful as well as useful information.
I read a study that evaluated time lines of autophagy and mitophagy during a water fast. Mitophagy peaked at 24hrs and then there was a significant drop off. So during my water only fast day I take NR.
I avoid all AMPK activators on those days however since a study showed that AMPK negatively effects mitophagy. Faseb,J. AMPK Negatively Regulates Mitophagy. April 2017 31 (1) supp 634.1
As you know, I’m all in with rapamycin, but I wonder along with you if hitting it harder but less frequently may be better. It also does seem to make fasting easier.
I agree with your final assessment as it pertains to any one substance or intervention, but I have come to believe that multiple approaches utilizing synergy at suboptimal doses and through complementary pathways is now the way to go. I believe that that approach will ultimately yield more than healthspan alone.
At least that is my fervent hope.
I don’t believe that study Paul. AMPK downreglating mitophagy just doesn’t make any sense to me. You’ve got interactions between AMPK, MTOR and FoxO3a all tipping the scales to and fro on mitochondrial biogenesis vs mitophagy. I think it’s more likely mice lacking AMPK are increasing MTOR, which is creating more mitochondrial mass, and maybe another pathway to mitophagy like FoxO3a is trying to get rid of the excess in the liposomes.
Having said that, AMPK with NR might not be a great idea as AMPK can make new mitochondria as well (to avoid a further energy deficit), and during mitophagy you probably just want to be getting rid of the bad stuff without giving it any assistance. The key takeaway: mitophagy should make you feel pretty bad.
Thanks
That makes a great deal of sense.
I’ll stop worrying about AMPK on fasting days.
I do actually feel pretty bad between the 20-24hr interval of the fast. My colleagues say that it goes away by hour36-48 fast, which is precisely when mitophagy returns to baseline. They also claim that by day 4 they feel really good.
Crazy.
That matches with what I’ve experienced (just using Nicotinamide and D-Ribose). A day of feeling bad, then an okay day or two, then bounce back and feel great.
So you could try with and without AMPK activators. it should be pretty obvious if AMPK activators are stopping it working. One confounding factor, repeating this protocol diminishes the effects, as you’d expect as you decrease the pool of bad mitochondria.
Hi Mark,
I agree with your statement about impact of CR / Rapa in humans. It is likely more about health span than max life span. Primates studies have showed that CR do not increase LS in similar proportions than in mice. I don’t expect the impact to be completely 0 in humans though as it would be a weird phenomena but maybe around 3 to 5 years of max LS increase.
The health span effect looks very substantial in itself though. Alan and Paul have reported great benefits with Rapa on several parameters.
I see mTOR inhibitors as a great first step, a proof of concept that aging is not immutable, before more powerful anti-aging treatments capable of addressing the post-aging syndrome are available, possibly in the 22 century but hopefully a bit sooner.
Just to clarify, when you say increase max lifespan do you mean beyond 120 years in humans? So maybe 123-125 y/o with present methods?
I agree Aldebaran. Today I see maximum lifespan 101. So maybe few people live to 104.
Goal of anti-aging is to be healthy 8th and 9th decades of life.
Nobody is getting out of this alive; the bad part is 20 years of pain and suffering.
But our max lifespan must be beyond 101, didn’t the oldest man just die at almost 114y/o?
Hi Paul,
You are correct.
The oldest living man, the Aushwitz survivor just died this past September, one month before 114 birthday.
By maximum lifespan I meant oldest 1-2%.
I do think will see is dramatic increase in mean lifespan and lifespan oldest 10% of people on anti-aging plans,
Hi Paul,
Good question. I prefer max LS defined as
the mean life span of the most long-lived 10% (or even better as Alan suggested the most long-lived 1% if we have a large sample).
So with this definition, if we have two groups of people of age 60 and we give rapa to group A and placebo to group B for the rest of their lives, my guess is that max life span of group A would be 3-4 years higher than max life span of group B and mean life span of group A would probably be more like 6-8 years higher than group B. Of course this is just pure speculation but if this is close to correct, it could have a massive impact on aging distribution. And I am not mentioning health span which is probably even more important.
The usual definition of max LS for human which is the age at which died the oldest human is more about outliers than about the distribution of LS. We are not suddenly aging slower since 1997 because Jeanne Calment has raised the max life span from 117 to 122.
Hi Alan,
I agree that quality of life of 8th and 9th decade is an extremely important point. If rapa can deliver on this alone, this is huge.
Hi Aldebaran
I feel like it should do more than that . I should be able to attain that goal with supplements, IF, and diet/exercise. I want rapa to get me to 120, ( but that might mean synergy with something else). Bill Andrews says that he’s going to be immortal even without rapamycin, just by messing with his telomeres.
Hi Paul,
I certainly don’t disagree.I was just considering a very conservative hypothesis but my current guess is rapa should significantly extend both max and mean LS in human.
My guess is that rapa will allow you to reach 120 if you would have reached 110 without rapa. But it could be more than that as well.
Paul,
Also, is it fair to say that you and Alan have experienced a significant improvement in cardiac capacity with rapa which is probably not achievable with supplements alone?
Paul,
Rapamycin is slowing down proliferation of cells (so preserving telomeres), and decreasing the pressure on arrested cells to become senescent (which makes us old/unhealthy).
Ideally we shouldn’t have to care about this. Just let senescent cells be cleared by a functioning immune system and be replaced by other cells with protective long telomeres and youthful gene expression.
But we are where we are in aging research and must look to slow aging down until we have better treatments.
I think many of us commenting here have essentially solved ‘healthy aging’, which is often considered some sort of Holy Grail. But the real Holy Grail is yet to come.
My guess is that I have a 50% chance of making it to a point where aging is postponed long enough for it not to be a factor in my mortality. I think for my children it is more like 90%. I base this on the absurdly fast progress being made in science in general, and biotech specifically.
Hi Mark,
I don’t disagree. You are in the optimistic camp but nothing of what you say seem surrealistic to me. It all depends of future progress. Cannot wait to see the state of epigenetic reprogramming in 20 years!
Paul,
I would really like Bill Andrew to be right but how can just extending telomeres be enough to live much longer? Don’t we need also to reset at least some epigenetic changes as well to get a substantial effect on aging? Now, Bill Andrew knows much more than me on aging so maybe I am missing something.
Of course you make a great point Aldebaran, and I need to read his new book, but I know at one time that he was really into telomeres and lifespan. Not sure what he thinks at this point.
Aldebaran, I haven’t read Bill Andrews new book yet either, but I think he and Michael Fossel are probably right that lengthening telomeres is the best intervention against aging that is currently or soon to be available. I am referring here to a genetic one off or occasionally repeated therapy that lengths telomeres.
Telomeres regulate many genes and as they shorten gene expression changes. So it is not just a matter of replicative senescence. There are many good papers by Shay and Wright on this phenomenon. So what does lengthening telomeres not do?
There are other epigenetic changes outside of that regulated by telomere length, but these changes seem to be very subtle and are not proven to be detrimental at this time. Although I suspect eventually we will have to deal with them too.
Also, non cycling cells degrade too by other mechanisms. However, this may be in part due to the decay of proliferating cells. The example Michael Fossel gives is astrocytes are the main cause of neuronal decay. Again, I think this is not 100% of the reason, so we will have to deal with other issues, but for now telomeres are absolutely the way to go.
Hi Mark
New project working on is prevention AD in carriers of ApoE4 allele. Aside from 2% of genetic early onset cases, AD is 2 hit disease with first hit being microcirculation and breakdown of BBB and decrease in perfusion. Second hit the amyloid cascade. As regards astrocytes, no; but pericytes which form major part of Neurovascular units are major cell player.
Mark,
Interesting point about telomere. I will look at papers from Shay and Wright to better understand.
Yes, Mark. I will be taking my dose of Rapa once per week as that seems to be the most common frequency. My first two weeks, I took two milligrams. The next two weeks I will again be taking two milligrams but will be taking with grapefruit juice (fresh) as it has been found to increase potency by upward of three hundred percent.
Hey Larry,
Grapefruit juice turns Rapamycin into a poison. Number one warning about Rapamycin is don’t take with grapefruit juice.
Rapamycin is not a food supplement. It is a very potent and dangerous prescription drug for good reason.
Thank you Alan. I will follow your advice..No more grapefruit juice.
A recent double blind placebo phase II human clinical trial in Miami showed heterochronic mesenchymal stem cells single dose creates substantial recovery from age related frailty. I am unable to post the link so Google. It has proven safe and significantly rejuvenative. If Phase III succeeds this can win FDA approval which would quite an achievement in aging research.
Hi Akshay,
Thanks. Looks like a very interesting finding!
Just started to read the following editorial related to the study you have mentioned:
Stem Cell Transplantation for Frailty
David G Le Couteur, MD, PhD Rozalyn M Anderson, PhD Anne B Newman, MD, MPH Rafael de Cabo, PhD
The Journals of Gerontology: Series A, Volume 72, Issue 11, 12 October 2017, Pages 1503–1504, https://doi.org/10.1093/gerona/glx158
Thank you Aldebaran. The immense significance of these trials is that even though we have seen many many anti aging successes in mice and worms none have so far translated to humans proven irrefutably in clinical trials that can achieve FDA stamp of approval. Although, this has not yet conducted Phase III so let’s pray it clears this penultimate milestone as well. Having said that the challenges are finding young donors ready to go through the very painful bone marrow extraction and the second would be the cost. If it does get the FDA approval then I am sure there will the rich who will want to get the benefit.
Does it have to be bone marrow Akshay? What about umbilical cord?
I had got excited about cord blood when I was researching on heterochronic transfers but then I came across mixed studies – if I remember correctly it led to cancer. So I immediately stopped in my tracks. So I don’t know if any successful studies have been demonstrated in cord blood stem cells.
Cannot they use a few numbers of donors and replicate their MSCs in vitro indefinitely?
Are you aware of any LS extension obtained with IV injection of MSC in mice?
We will see how long the benefit of MSC last. I am not sure if they can replicate after transplantation.
If it reversed frailty then it can’t just be a signalling thing, the stem cells must have taken. But I’ll wait to read the full paper when it’s available.
I think your idea is a good one. I read a paper recently where they used a new RNA method to extend the telomeres in cultured cells, and it was incredibly quick and efficient. So much so that it was heralded as an easy way to develop lots more cell lines. So this could certainly be done from a small sample from a donor.
Nice that the paper is open access:
“Allogeneic Mesenchymal Stem Cells Ameliorate Aging Frailty: A Phase II Randomized, Double-Blind, Placebo-Controlled Clinical Trial ”
Two possible caveats are the small number of patients (10 in each group) and the fact that the group 100M did better than group 200M. They explain possible reasons why. A larger study is planned so looking forward to see that. Looks very interesting to me overall.
Hi Mark,
In regard to telemeres and AD, I came upon this paper thought you might find interesting, “Telomere shortening REDUCES Alzheimer’s disease amyloid pathology in mice.” 2011, Brain, Rolyan, “Telemere shortening…can slow down the progression of amyloid plaque pathology in AD, possibly involving telemere-dependent effects on microglia activation.
Previously I had pointed out that the novel idea of curing AD by increasing length telemeres by gene therapy was total nonsense. Most studies have no effect of telemeres in AD pathogenesis.. This study finds shortening telemeres is protective. Apparent mechanism is telemere enabled glia inflammation worsens disease.