
In the 1980s, Growth Hormone was explored by athletes to build muscles and by aging men to…build muscles. GH made them feel younger, revived energy and sex drive and even cognitive performance. Then the other shoe dropped: Animals without the GH receptor lived longer, while animals with extra copies of the GH gene die early. GH and IGF-1 are associated with higher rates of cancer, both in humans and in animals. Now there are credible scientists seeking ways to separate the benefits of GH/IGF from the tradeoffs. A prominent NIH research group suggests we can activate IGF-1 in some tissues and not others. In preliminary experiments on himself, Greg Fahy has regrown thymus tissue with GH and DHEA. Rhonda Patrick recommends saunas and weightlifting. Examine.com suggests supplementing with creatine as another option.
HGH (human growth hormone) and IGF-1 (Insulin-like Growth Factor) are closely related steroid hormones which stimulate muscle and bone growth. GH is produced in the pituitary gland, deep in the brain, and it circulates through the blood to the liver, where it stimulates production of IGF-1. In addition to the liver, there are local producers of IGF-1 in the body and the brain. Most of the effects of GH are mediated through IGF-1. Here is a good basic reference. A few years ago, Journal of Gerontology devoted a special issue to IGF-1.
IGF-1 is part of an ancient signaling system that promotes growth and depresses life span across many species. The system includes insulin, a protein structurally very similar to IGF-1 (hence the name). Insulin is a mediator of life span regulation through food, exercise and the energy metabolism. Some proteins carry instructions in the blood; they attach to receptors on the surface of a cell and tell the cell what to do. Others get inside the cell and play a more direct role in the chemistry. IGF-1 does both. It has “both endocrine and autocrine functions”.
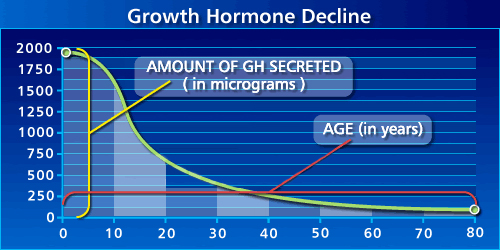
We have a lot more of both GH and IGF when we are growing children than later in life.
This discovery in the 1970s led medical researchers and others to the hope that HGH might be a kind of youth serum, and it was explored as a treatment for weakness, low energy, and depression in the elderly. It worked. IGF-1 combats the loss of muscle mass in old age, both by promoting new tissue growth and retarding apoptosis (cell suicide that protects against infection and cancer, but that can kill healthy cells as we get older). IGF-1 promotes new nerve growth in the brain, and has been linked to better cognitive performance as well as subjective feelings of youth and wellbeing.
But then it became clear that there are long-term risks associated with GH treatment, and GH treatment began to decline before it had really taken off. In the 1950s, long before genetic engineering, the Ames Dwarf Mouse* was as a mutant strain. It lacks the gene for GH, and it lives 50% longer than other mice of the same species. Other mice with GH or IGF deficiencies live longer, while mice with extra copies of these same genes have shorter life spans. [ref, ref]. But the results of lower IGF aren’t all good, and they don’t apply in all rodents [ref]. In dwarf mice, low IGF leads to insulin resistance, diabetes symptoms and cardiovascular disease when the mice are fed a high-fat diet [ref]. IGF-1 protects heart and arteries from deterioratation with age [ref].
“Despite the compelling data for enhanced life span in the presence of GH and IGF-1 defiiency in Ames dwarf and Snell dwarf mice, a review of the literature indicates that the effects of GH/IGF-1 defiiency on life span in many other rodent models are, in many cases, inconsistent…Thus, despite the general consensus that the GH/IGF-1 pathway is a conserved mechanism of aging, the data for increased life span in response to manipulation of this pathway in rodent models remain inconsistent and appear to be the result of studies in an important subset of animal models.” [ref]
The story in people is even more complex. Laron dwarfism is a genetic defect in the receptor for GH, which interrupts the connection GH → IGF-1. Laron dwarfs have high GH, but low IGF-1. (They are treatable with IGF-1.) There is a region of Ecuador with a high frequency of Laron dwarfism [NYTimes article].

People with Laron Dwarfism Syndrome have symptoms of premature aging, including wrinkling and obesity. But despite high insulin, they never develop diabetes symptoms. What about life span? There are contradictory claims of longer and shorter life span for Ecuador’s dwarf population.
Caloric Restriction provides another signpost. Many hormone levels are affected by CR, and the direction in which they move is a suggestion about whether that hormone can be expected to be pro-longevity or the opposite. Luigi Fontana of Washington Univ of St Louis has been conducting a long-term study of people on chronic (voluntary) CR. He found that circulating IGF-1 levels are not different in this population. Protein restriction is another classical life-extensio diet, and Fontana found that protein restriction quickly causes IGF-1 levels to plummet [ref].
Are higher IGF-1 levels a risk factor for cancer in humans? Maybe–but the association is weak and statistics are subject to different interpretations [ref].
Classical Example of Antagonistic Pleiotropy?
The prevailing evolutionary theory of aging today is called “Antagonistic Pleiotropy” (AP). The meaning is that there are genes that have multiple effects at different times in life, forcing evolution to accept costly tradeoffs (later) in exchange for peak fitness early in life. IGF-1 is frequently cited as a prime example in support of the AP theory. Evolution has selected IGF-1 in order to promote rapid growth, strength and development in youth, even though IGF-1 has long-term side effects that include cancer and higher all-cause mortality. IGF-1 signaling is a pathway that is conserved over a long course of evolutionary history, helping to reconcile evolutionary theory with the existence of tightly-related genes that regulate aging across the biosphere—a relationship that took theoreticians quite by surprise when it was discovered in the 1990s.
But a closer look at the biology of IGF-1 makes support for the AP theory more dubious. The details of where and when IGF-1 is expressed don’t fit the convenient story of AP. There is a lot of IGF-1 early in life, but no sign of deleterious effects. Later in life when the piper is to be paid, IGF-1 is expressed at very low levels. It is not easy to relate high levels of IGF-1 in our teens to the cancer and heart risk in our 70’s.
Also, experiments with “mosaic worms” have shown that the benefits of IGF-1 can be separated from the costs. “Mosaic” means that the worms have been grown with different genetics in different tissues. With this technique, it was shown that the pro-aging costs of IGF-1 are confined to expression in the nervous system, while the benefits come from expressing IGF-1 in muscle tissue. Why, then, has nature not found the optimal solution, and evolved worms to express IGF-1 only in muscle tissue?
HGH to Regrow the Thymus
The thymus is a tiny gland where our white blood cells (T-cells) are trained to distinguish self from invader. The thymus shrinks through our lifetime, and its loss has broad consequences for all the diseases of old age–autoimmunity, weaker defense against infectious disease, failure of the immune system to eliminate cancer in its earliest stages.
Greg Fahy is an innovative biochemist and personal friend. When he was 46, he successfully regrew his own thymus in a short, one-man experiment using HGH and DHEA. The procedure was written up as a journal article here, and his patent on the procedure is here. For safety, he monitored IGF-1 levels to assure that they did not exceed those in a healthy, young adult. This year, Fahy is conducting a tiny clinical trial based on this experience.
Safe ways to enhance IGF-1? Maybe.
Rhonda Patrick gives a succinct and powerful case for an IGF trade-off: Better physical and mental performance vs shorter life span. She hints that you might be able to get the benefits without the costs with natural means of enhancing IGF: physical exercise and saunas. Physical Exercise is a safe bet, because we know there is a net benefit for longevity, as well as abundant health benefits in the here and now. Saunas (“hyperthermic conditioning”) also boost the body’s own HGH without injecting anything. Heat shock has a hormetic benefit for life span in rodents and especially in worms; but I know of no epidemiological evidence linking the result to either a longer or shorter life span in humans.
Creatine is a small molecule, a substance that we all have lots of in our bodies already, though less as we age. It is a popular supplement among body-builders. Creatine acts in some of the same anabolic pathways as GH, promoting muscle growth. Creatine acts by inhibiting myostatin, which is a growth inhibitor, so it is the sort of double negative that makes for grammatical awkwardness. Eating creatine triggers a burst of GH release. Regular use of creatine boosts the background level of GH, but actually suppresses the burst of GH that comes with exercise.
In an an article from researchers at the Reynolds Oklahoma Center on Aging and National Inst of Aging, researchers suggest that it should be feasible to tease apart the benefits and costs of IGF-1 by raising IGF-1 preferentially in some tissues and not others. DAF-2 was an early life extension gene in worms–disable it and the worm lives twice as long. So what’s the counterpart of DAF-2 in humans? Turns out it’s an IGF-1 receptor. A few years later, Gary Ruvkun discovered that disabling DAF-2 in just the worm’s nervous system was sufficient to extend life span. This suggests that it might be possible to de-couple the anabolic benefits of IGF-1 from the life-shortening consequences. If people are like worms, that is…
—————
*named for Ames, Iowa, not Bruce Ames
Discover more from Josh Mitteldorf
Subscribe to get the latest posts sent to your email.
I remember reading a paper according to which there is a very strong GH surge after refeeding from starvation. (Also this GH surge could stimulate transplanted tumours in animals.)
I have long contemplated how the periodic fasting by Longo has its effect through restriction of IGF-1 when in the refeeding period there is a strong surge in GH. I couldnt understand. Maybe I will understand more after reading the references.
Hi Josh
Good to read this briefing on the effects of HGH & IGF…Bu I suggest that a lot more could be said. We know that a large number of individuals have been taking HGH on the recommendation of some anti-aging doctors since the early 1990’s. Surely by now there is some evidence of 1) whether HGH has anti-aging effects in these individuals and 2) whether substantial numbers of these individuals have been impacted by cancers as a result..AS for me it seems that creatine is the way to go.
Melatonin + exercise is another path that I can recommend.
link
Here is an article finding life extension for mice that received life-long, low-level injections of GH.
I am not aware of on-line listserves where people taking GH share their experience, but I agree with you it is likely that they exist.
I use creatine, ALA , astragalus and Glycine myself and Creatine for sure has increased my energy and improved muscle.
how old are you
Hello dear Josh,
I am suffering from hypothyroid ( taking75 mcg Thyroxine medication), on the mean time I am too low in HGH ( almost zero in all provocative pituitary blood test. I am using 1 iu every other day and the fatigue is still there. My Igf1 jumped from 180 into 225 and I am 42 male.
Please advise if you think I might need to go for 1 iu daily. The local doc is saying it is enough, me however still suffering from weight gain and chronic fatigue.
I know you don’t prescripe medication, just I need your opinion.
Thanks,
Dear Josh,
Thank you for your interesting article. Based on the work of CYnthia Kenyon, I have been interested in activating the FOXO repair mechanisms via inhibition of the PI3K-AKT pathway. Blocking this pathway triggers repair.
However, The PI3K pathway is triggered by IGF1 and by insulin – both necessary for growth.
The reason why IGF1 can shorten lifespan is because it upregulates growth at the expense of repair.
However, my plan is to apply both in a cycle. 2 days of high protein/creatine flowed by 2 days of fasting/ parthenolide (parthenolide is a powerful inducer of autophagy and blocks PI3K pathway by blocking IRS1)
That way, I will get all the benefits of IGF1 whilst also getting the repair. HEnce my lifespan and Healthspan should be maximal.
I discovered that Parthenolide was such a good activator of autophagy and blocker of PI3K when I compared the gene expression profiles of different drugs with the gene expression profiles of autophagy and of the PI3K pathway. Parthenolide came out top.
See – https://youtu.be/_2r9D03nDZY
I have been taking Parthenolide, which induces autophagy and blocks the PI3K pathway
> catabolic pathways
Not to risk sounding like an ignorant gym rat but… shouldn’t it be ‘anabolic’ pathways? 🙂
Thank you! Without a staff, I have come to count on perceptive readers to catch me in proof-reading errors like this and in bigger mistakes as well – whole areas of the literature that I may be unfamiliar with.
I’ve read somewhere that the half-life of synthetic HGH has been extended above that of the natural HGH. It seems logical that the burst of HGH for intense exercise would have much less potential for negative effects than synthetic HGH. Not only the half-life but also the HGH can be put to work immediately in the body rebuilding and repairing the damage from exercise.
Also, what about A_GPC for HGH release?
Josh,
Thanks for your well-written post!
For life-span effects of Sauna, I would like to add a reference:
Association Between Sauna Bathing and Fatal Cardiovascular and All-Cause Mortality Events
http://archinte.jamanetwork.com/article.aspx?articleid=2130724
Good to know since I like the sauna.
However, I also wonder if exposure to cold would also be beneficial.
Seems to be a question of health span versus doing nothing (which we know what the outcome of doing nothing is). Look at Sylvester Stallone…. he admits t taking growth hormone, and he is going along just great in his late 60s. I would use his example to make my point of health span versus doing nothing. Maybe he won’t live to be 120 because of the GH, but so what? Who does? And what’s the quality of life? I’d rather have a health a vitality span into my 80s only to drop dead than to have a health and vitality span into my late 50s early 60s and then wither away. Who wants to live to be 120 if you are bound to a bed? I choose quality over quantity.
This is all anecdotal, I admit in advance. I have experience with being off and on HGH and it’s effects. I am an OBGYN in solo practice for 30 years. I am 55 now. Ten years ago, after 13 years taking call every night for myself in a busy one man practice, I felt like a truck hit me. I was evaluated and trained at The Cenegenics Medical Institute. I found my testosterone was 275, normal for a 72 year old at 44. I knew this had to be from a lack of sleep, but that was something that could not change overnight. I started testosterone supplementation and HGH. I felt better overnight. I felt like I was a teenager again. All my friends and family noticed and mentioned it. The other dads on an annual ski trip were amazed I was the same guy as the prior 5 years. All my middle age aches and pains were gone.
For the prior six years, I had worked out 4 days a week with a personal trainer and got ZERO results due to my lack of hormones. I was extremely frustrated. I was not working out at the time. In the first year, I lost 13 pounds of fat and gained 12 pounds of muscle, just by fixing my hormones. No change in exercise or diet. The strangest thing was my hair turned curly, much more so than in my youth.
I took the HGH daily 2006 through 2010. Due to the expense, $700/month, I was off and on for a couple of years. I experienced a decline in my physical condition. In 2012, I decided to get serious and restarted HGH. I began working out 5 days a week. 2012 and 2013, I was in the best shape of my life and felt like a teenager. On testosterone, HGH, eating right and working out extensively the fat melted off my body. I went from 19% to 9% in a couple of months. I was 50 at the time. I was a HS athlete and competitive weight-lifter. I was in better shape at 50 than in HS. When I saw people I had not seen in a while, they did not recognize me. When I spoke and they knew who I was, they looked like they had seen a ghost. I am not exaggerating.
In 2010, I was diagnosed with severe sleep apnea. In 2012, I was diagnosed with delayed sleep latency onset, meaning my brain acclimated to being paged several times a night by not allowing me to go into REM sleep. I stopped taking call. It took me a full three years to start dreaming/have REM sleep again.
I used HGH through 2013. First, they increased the price 50%, then the FDA stepped in. The FDA made obtaining HGH very difficult in 2013-2014. I got off in 2014. I have received a waiver due to my REM sleep problems. I would like to restart HGH as I have seen an appreciable decline in my physical condition since 2014. Testosterone helps, but testosterone and HGH are magic.
Anyway, that is my anecdotal experience.
Thanks for most useful post
Have you heard of the Homeopathic HGH GEL it’s FDA registered
Chris, Thanks for your post, really helpful. I am 45 and started taking HGH 3.5 iU daily at night. What dose did you take 2012 2013?
Hi Chris,
You might want to try HGH activity 8 and an IGF-! spray!
My diabetes has vanished and have lost 10 lbs in a couple months.
I am a 74 year old MD working like a 40 year old!
Thanks Chris for sharing. I am 45 of age and started taking HGH 3iu daily. Today 2 month ago I started and have had some amazing loss of fat, just concern on the cancer and life span information on the web. I would like to share some thoughts and would like some advice, will try to reach out for you. Best.
Has anyone heard anymore about Fasting and IGF1? I am fasting to help Prostate issues and overall health and immune system. However, I have read studies where high levels of igf1 are implicated in prostate cancer.
1. Am I defeating my purpose by fasting?
2. I believe in all of the benefits of fasting, but concerned it may be a two edged sword in my case?
Any related info or input greatly appreciated.
What about teens heading into puberty who are low on GH? My 14 year old son’s thyroid and pituitary function seem normal, but he is low on GH. His doctor wants to start him on synthetic GH which makes me a little nervous. He is producing growth hormone, but it’s just below the level it should be. A friend was telling me that my doctor should’ve tested for IGF-1 instead of HGH. Not sure if this is accurate or not?? Anyway, do Saunas and Creatine work in this type of situation? Trying to find natural ways for him to boost GH without going the synthetic route. I’m wondering if his GH levels might increase as he heads more into puberty?? He hasn’t shown any real signs of puberty yet, but his doctor says he’s in the initial stage. A little background: he used to do heavy endurance exercise (cross country mountain biking), which we had him stop in exchange for weightlifting and football. He has upped his protein intake by drinking pea and whey protein shakes everyday in addition to his normal meals. His doctor recommended he have around 70 grams of protein per day.