
Deprenyl is a neuro-protective drug discovered in Hungary more than 30 years ago. It has prolonged life span in many rodent studies, and also in dogs. In the 1990s, under the brand name Selegiline(also Eldepryl and Zelapar) it became a standard treatment for Parkinson’s Disease. Parkinson’s patients who take Selegiline live longer than matched patients who take only the other standard treatment (L-Dopa). More recently the same drug (branded as Emsam) has been prescribed for depression and ADD. There is a small cult of people who take it daily for life extension, with good rationale (in my estimation). But it has an effect on mood and personality that not everyone will appreciate.
Medical literature classes deprenyl as an MAO-B inhibitor. What does that mean?
For non-specialists, the story should start with neurotransmitters. The electrical network of the brain is modulated chemically by neurotransmitters that determine how easily and strongly its signals are transduced. Dopamine, adrenaline, melatonin and serotonin are all common examples of mono-amine neurotransmitters, named for a chemical structure they have in common. Neurotransmitters are constantly being produced in response to stimuli, and broken down so their levels in the brain can be adjusted from moment to moment. The breakdown is accomplished by an enzyme called a mono-amine oxidase. There are two closely-related forms of these breakdown chemicals, known as MAO-A and and MAO-B. Type A breaks down all four of the MAO’s listed above. MAO-B specializes in dopamine.
Two important things to know about dopamine are (1) that it’s essential to the brain’s reward center that makes us feel good in response to social cues or sex or food or whatever, and (2) Parkinson’s disease is caused by death of cells in the midbrain that manufacture dopamine, so that dopamine levels are very low in Parkinson’s patients.
The last word in the description is “inhibitor”. “Mono-amine oxidase inhibitor” is a double negative – it prevents breaking down the neurotransmitters, so more of them circulates. Deprenyl in particular prevents the breakdown of dopamine.
Brain aging
All of this provides good support for understanding the function of deprenyl as a Parkinson’s drug and anti-depressant. But why should it affect aging? Why should it protect the brain? It has been known for 20 years that deprenyl protects nerve cells from toxins and even can help to rescue nerve cells after they have been damaged. Though the mechanism is not understood in detail, there are some clues. Neural growth factors have been found to increase in the brain. Superoxide dismutase (SOD) and catalase are part of our natural protection against oxidative damage, and and both these are enhanced in the brains of people taking deprenyl. Glutathione is another of the body’s natural protections which has been found to increase (in rats) in response to deprenyl. This same study found a larger density of neurons and better retention of learning abilities in deprenyl-treated rats.
Personally, I have never taken deprenyl. In fact, I’m a purist about the quality of my consciousness – some would say obsessively so – and I stay away from caffeine, alcohol and marijuana, let alone prescription anti-depressants. But I know people who have taken Selegeline as an anti-depressant, with results that seemed to me to be noticeable from the outside. With Selegeline, they were inspired to new creative projects, full of enthusiasm, less realistic about follow-through and detail. That’s my personal observation.
And here’s a red flag: Deprenyl metabolizes to methamphetamine. Though I have no personal experience with methamphetamine, it certainly gives me pause if I were to consider deprenyl for myself, or recommend it to anyone. Why is it that deprenyl seems far less addictive and less destructive to personality than methamphetamine? It may be because typical dosages of deprenyl are small compared to recreational dosages of meth.
Life extension
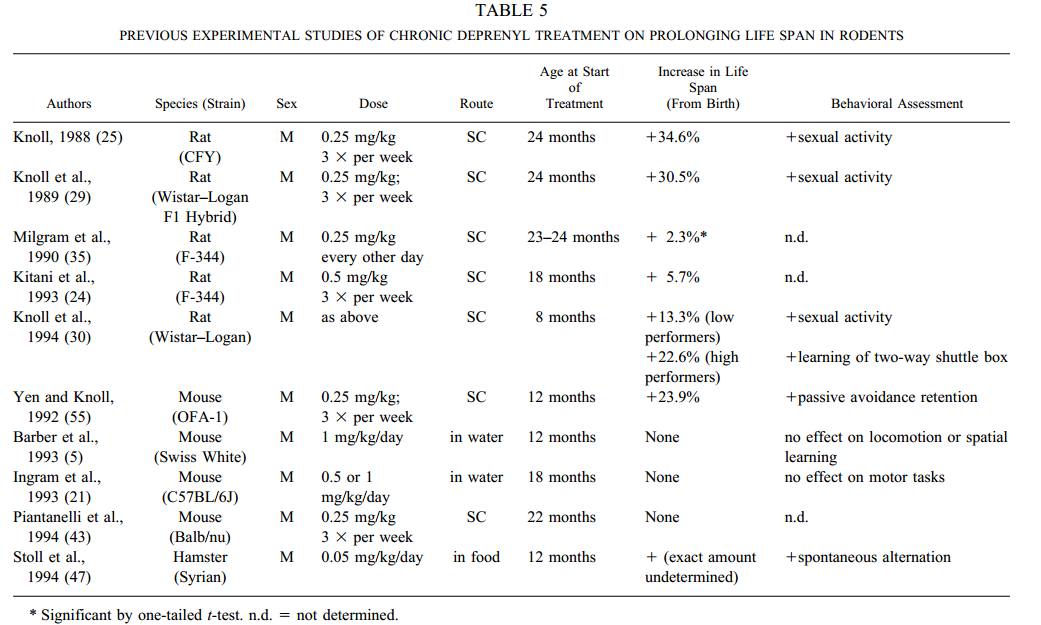
The first rat study was done in 1988 by Knoll himself (discoverer of the drug), with spectacular results. Though deprenyl treatment was not begun until the rats were middle-aged, the treated rats still lived 34% longer than controls. Subsequent rodent studies continued to show significant life extension, but no one found the dramatic results claimed by Knoll.
Why the difference in results? Part of the discrepancy may have to do with dosage. High dosages of deprenyl can shorten life span, as reported by a Japanese group in 2006.
There was one study on dogs, significant because dogs live longer than mice or rats, and caloric restriction (CR) is proportionately much less effective in longer-lived animals. Does deprenyl behave like CR, with proportionately smaller effects in long-lived species? The results from this one experiment give a tantalizing suggestion: perhaps not; but the study was terminated too early to offer a quantitative estimate of life extension. The study included 33 dogs that were more than 10 years old when they were first placed on deprenyl, but the study was terminated before most of the dogs died, making it difficult to estimate the life extension benefit. 80% of the deprenyl-treated dogs survived to the end of the study, but less than 40% of the untreated dogs.
We can’t help but get the impression that deprenyl has a lot of potential as a life extension drug, and that the subject cries out for more research. Knoll has come out quite explicitly recommending deprenyl as a generalized anti-aging tonic. Most of the nutritional interventions that we know about that extend life span in animals work through the insulin pathway that governs the caloric restriction response. This may mean that simultaneously cutting calories while taking resveratrol and metformin has less benefit than what you might expect by adding the benefit of each of these separately. Deprenyl, however, seems to work through an independent pathway, so there is reason to hope that whatever longevity gains it offers are in addition to those from caloric restriction and CR mimetics.
Why?
We may be surprised that a stimulant can lead to longer life. What happened to “Speed kills”? Most of our intuitions about the rate of aging are based on the idea that the body is wearing out, and faster we move, the quicker we wear out. This is the “rate of living” hypothesis, which is discredited, as as I wrote a few weeks ago. We should remember that physical activity leads to longer life span. We should think in terms of hormesis – the body’s paradoxical response to hardships and challenges. In fact, deprenyl extends life expectancy in small doses, but is toxic in higher doses – the signature of hormesis.
Is this for me?
People taking deprenyl for life extension report palpable effects on mood and energy. Meanwhile, the impact on life span is distant and largely untried in humans. If you like the way deprenyl gives you more energy, more enthusiasm, more ideas, then the thought that this drug may extend your life is a nice bonus. If you find that the drug makes you nervous and raises anxiety, if you lose sleep and are separated from your inner being, then tipping your odds for future longevity will not be worth it.
Just a few days ago, I received a missive embodying the wisdom of the East. It came from a fortune cookie at my local Chinese take-out, and its message read: “The quality, not the longevity of one’s life is what is important.”
For basic information about healthy living for a long life, see the author’s permanent page at AgingAdvice.org.
Discover more from Josh Mitteldorf
Subscribe to get the latest posts sent to your email.
The reason the presumed effects of the metabolite methamphetamine aren’t noticed is that the active drug form of meth is D-methamphetamine, selegline/deprenyl metabolizes into L-methamp which doesn’t give the same euphoric effects.
Thank you! I hadn’t realized that it was an enantiomer, rather than the biologically active isomer.
I’m 63 m. I have no pain and feel 21. I lived an abusive life style drinking 35 years an average of 16 oz. of rum a a day and other stuff, stopped at 61. The last 20 years I have also ate for health, avoiding junk, sugar and going organic. I had a bad back in my 20’s to 30’s which was sore and would cramp up at times. I started taking deprenyl at 40, one year later my back cleared up and since then it never bothers me. I had planned to take it for 30 yrs to see what would happen and no other reason. I will continue to take till I die into my hundreds. LOL
hi ,
i am going to start taking deprenyl tablet form for longevity etc what dosage do you take per week ?
i am 45 now so little bit later than you i have read some articles they differ slightly some say 7.5mg per week others 10/15mg per week .
thanks
I started out with the liquid form of a citrate which can’t be found now. I took 1 mg at 40 yr old per day then added one mg for every 5 years. Now I just a 5 mg pill once or twice a week. Prof Knoll who founded it revised his dosages and in his 80’s I think he only does 1 mg/day.
good for you to quit the junk before it kills you. Those things alone will make a person feel better. I want to feel well also. I take 5 mg in morning only, and notice a difference, I am 81 and will take it as long as I can get it. I am concerned about the possibility of interaction if I have to take a pain medication. such as dilaudid 2 mg. Deprenal is no longer listed in the PDR book.
There were reports that Deprenyl shortens lifespan, and also reports that it increases lifespan. The unsaturated substituent at Deprenyl’s nitrogen can get peroxidized, so I would not recommend Deprenyl. Take Adderall – it is amphetamine, which rejuvenates if taken systematically e.g. 30 mg/day.
How possible is it to procure Deprenyl without a doctor’s script?
Since you’ve begun taking this drug, what are your thoughts on it?
Hi: Since the Japanese study showed that high dose dephrenyl could reduce lifespan in mice, what would be the dose in humans that can have beneficial effect. It is often very hard to translate mouse dose into human dose because they have different metabolism and drug detoxification rates than humans (even absorption is different). Since there are a few Dephrenyl users here who take the drug for longevity and improved neurological health, can anyone advice?
There is no definitive information on this, as you suggest. For myself, I take 2.5mg three times a week. I am guided partly by the effect on my mood. If I take full 5mg pill, I can feel a little lightheadedness, like a sugar high. I don’t feel anything from 2.5mg.
Thanks a lot for the information on the dosage. It helps.
The Japanese study that I mentioned was from this article, which is http://www.ncbi.nlm.nih.gov/pubmed/16804014. It says. I didn’t have access to the full article, but the abstract says that anything over 0.5 mg/kg in mice shortened life-span while at or below 0.5 mg increased life-span.
To put this in context, there is lots of room between 0.5mg/kg and usual doses of Selegiline in humans. Typical doses used in the life extension community are 0.01 or 0.02 mg/kg, which are 20 to 50 times smaller than the dose that causes shortened life span in mice.
0.5mg/kg for a mouse equates to 0.04mg/kg for a human, or 2.8mg for a 70kg human, very close to your dose of 2.5mg. However, the mouse studies that I’ve seen were with injected deprenyl (not oral). Knoll’s 1994 study used 0.25mg/kg subcutaneously in rats, which would also equate to 0.04mg/kg in a human.
Presumably you’d need more oral deprenyl to equate to injected. The dog study I found used oral daily deprenyl tablets, 1mg/kg. That is a much higher dose– translates to 0.54mg/kg for humans, or… yikes… 38mg/day.
hi, i’m confused, it says in the article that you have never taken it?
At the time I wrote the piece I hadn’t taken deprenyl.
– JJM
hello!
Looking into this a bit, it looks like at larger doses, at least, you have to be quite careful about other meds, supplements and some foods or beverages that contain high amounts of tyramine (aged cheeses, sauerkraut, sausage/salami, soybean products, tap beer,…). This was when used transdermally at 6-12mg/24 hours) (see emsam sites).
Also, as an MAO inhibitor, does that make it anticholinergic (which seems to up your chances of developing dementia)?
Josh,
I was wondering if you have an opinion of deprenyl’s anti-aging potential vs those of other MAO-B inhibitors that have come along since deprenyl’s development, such as Rasagiline, Ladostigil, and BPAP?
Matt
AFAIK, deprenyl has been validated in mice, with modest life extension, and these newer drugs have not been tried, or else they have been tried and the data hasn’t been reported. If you can find rodent data for any of these drugs, I would be interested to pass it on.
Unfortunately, all I’ve heard so far is anecdotal, pertaining more to Parkinson’s than to longevity, and thus not enough to act on. Theoretically, though, it sounds promising for longevity, especially regarding Rasagiline. I’ll keep my eyes open for any studies that may surface.
Tyramine is a concern with MAO-A inhibition while Deprenyl is generally an MAO-B inhibitor below 10 mg/day and somewhere in the range of 10-20 mg/day begins inhibiting MAO-A. At the dosages being tried for life extension, tyramine shouldn’t be an issue.
If Parkinson’s patients do indeed live longer than age matched controls, then one has to consider that they are taking well over the amount considered too high for life extension yet still getting life extension results. The amount of Deprenyl taken daily by them is much much higher than the 0.5-1.0 mg/day life life extensionists are taking so it seems that the amount where life span get shorted doesn’t align well with rodent studies.
Great read and following comments. I have recently started taking Selegeline a few months ago at a dose of 1 mg, 4 times a week. I am 41 yr old female 112 lbs. No negative side effects. To add to the conversation I would like to share a few links I found interesting which discuss the antioxidant and longevity pathway signaling functions which depreynl activates.
http://www.ncbi.nlm.nih.gov/pubmed/22019741
http://www.ncbi.nlm.nih.gov/pubmed/16325767
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3092636/pdf/nihms277305.pdf
Cheers.
Hi A.E. Trinh,
So no negative side effects, how about positive ones? Can you share what you’re noticing if anything?
thx : )
My guess is that the psychological effects are very individual and subjective. I found when I first took it that I thought I detected more friendliness, less social inhibition. For me, that’s a good thing. I have always taken a subclinical dose, 1mg per day or less.
I have no side effects at all – neither positive/negative. It’s very possible personal body chemistry makes a difference, as well as personality in general. Upping the dose to 2mg twice a week might produce elevated mood/energy for me, but that’s not my goal with taking Selegeline, also more does not always equal better.
Taking deprenyl greatly increases the activity of superoxide dismutase (SOD) – an antioxidant naturally produced in our body. This may sound like an added benefit, however at higher concentrations, antioxidants can become prooxidant — producing more free radicals than they neutralize
Even low doses of deprenyl can increase SOD resulting in higher levels of hydroxyl radicals which are notorious for attacking the deoxyribose DNA backbone causing damage that is toxic or mutagenic to the cell. This is why our endogenous and exogenous antioxidant systems must be kept in balance. Included in my daily stack are N-Acetyl-Cysteine (NAC), vitamin C, and vitamin E – all of which help offset elevated SOD activity.
To put my response above into context with active links, see full text here: http://secretforlongevity.com/experimental-and-controversial-deprenyl/
Selegiline metabolizes to LEVOmethamphetamine which is a stereoisomer thus not completely identical to common methamphetamine which is usually DEXTROmethamphetamine.
https://en.m.wikipedia.org/wiki/Levomethamphetamine
Has deprenyl ever been studied for its neuroprotective or possible neuro-rescue effect when administered after neural injury or insult such as infarct, ischemic or traumatic injury and in exposure to neurotoxin other than the one cited by the article?
What are the ethical concerns in giving human subjects a drug without indication for its use? (Not suffering from major depression, ADD, or Parkinson’s) How do those taking it solely for potential life extension get their supply?
I had a nerve injury occur to my urethra which manifests in painful symptoms only on the head of the penis. No inflammation, just a constant feeling of itching, scraping, or gnawing painful anxiolytic effects. 10 mg in the morning seems to help, and I feel great after taking it. I am thing of trying 15 mg to see if I can eliminate pain completely. Does anybody know if this can help pudendal neuralgia. This occurred after an artificial sphincter was placed in scrotum to control incontinence. Acts like a blood pressure cuff to cut urine on and off from leaking.
I have not bought or taken selegiline, but you could try this:
http://www.antiaging-systems.com/50-deprenyl?Aff=QCom
deprenyl does nothing special, it works by upregulating the nfr2 endogenous anti-oxidant system. which works for chemoprevention and neuroprotection (alzheimer,parkinson, etc). Can also be done with cucurmin, sulphoraphane, milk thistle. which also temporally increase ROS and the body reacts with more endogenous anti-oxidants. AMPK stimulators like aicar, metformin, salsalate also increase nfr2 but vis-a-vis comparison between ROS mediated nfr2 upregulation is not done in the literature(?).
https://www.google.com/search?q=nfr2+deprenyl&oq=nfr2+deprenyl&aqs=chrome..69i57.3500j0j7&sourceid=chrome&ie=UTF-8
Does anyone know anyone who has used Deprenyl for Dementia with Lewy Bodies (DLB)? DLB is sort of the complement of Parkinson’s disease. In both conditions, little lumps of something called Lewy Bodies appear in brain cells. DLB begins with cognitive changes and as it advances, physical symptoms develop. Parkinson’s develops in the reverse order: physical first, mind next. People with DLB are exceptionally sensitive to neuroleptics like Haldol, and should never use the drug. (Nor should anyone, in my opinion.) A bad reaction is suggestive of DLB.
I’m wondering if Deprenyl really is helpful in DLB. An article that said it is prompted me to search, and that is why I landed like a lead-filled dirigible on the outskirts of a conversation that started almost three years ago.
(If you do know anyone with PD or DLB, a recent results were encouraging. The tiny study didn’t get much airplay in the Parkinson’s world, maybe because it was small and was not a randomized, placebo-controlled study, or maybe because it rocks the boat. The drug, nilotinib (Tasigna® by Novartis®) is an FDA-approved for a type of leukemia, used at a low dose. https://gumc.georgetown.edu/news/Cancer-Drug-Improved-Cognition-and-Motor-Skills-in-Small-Parkinsons-Clinical-Trial
WHERE CAN I BUY DEPRENYL
With a prescription, you can get it in any drug store. It is sold as Selegiline (or Emsam transdermal). Without a prescription, you can probably get it through Canadian on-line pharmacies. If you have a doctor you trust, why not talk to her/him about it?
I’ve found PPAP HCl to be available for research. “Back of the envelope” figuring and Joseph Knolls’ findings suggest that ~1mg. sc daily would deliver deprenyls’ benefits with no possible MAO complications. At ~$40/gram it’s a bargain. Do you think this is a possibly fruitful stratagem for life-extension?
I have never heard of this, but I’ll look into it.
https://www.reddit.com/r/Nootropics/comments/4kl322/ppap_hcl_experience/
I recently had an 8 hour I.V. drip of NAD. I am neither a heroin addict, alcoholic or opioid dependent, but enjoy radical health excursions and experiences. My relationship to stress has really changed and I’ve cut my sugar intake over 95%. I’m now using NAD nasal spray. Does anyone have any thoughts on how this might work with or instead of deprenyl?
I am considering this also. What did you think about it afterwards?
Hi ginger; I have been interested in trying NAD+. Where do you get the nasal solution?
What dosage of DEPRENYL is recommended for a 75 year old female?
I think we’re in unexplored territory, extrapolating from a few small rodent studies.
Any thoughts on taking deprenyl as a means to treat ADHD and depression in an otherwise healthy 23 year old male? I am thinking of a very low dose of deprenyl 3-5x/week, but am unsure as to administer orally or sublingually as I know the ROA affects the metabolism of deprenyl.
On several occasions I experienced rejuvenation.
1) Excellent rejuvenation apparently caused just by severe
caloric restriction.
2) 25 mg to 50 mg of IMIPRAMINE daily + normal vegetarian diet
3) Caloric restrition + I guess about 30 mg of AMPHETAMINE daily.
I take this:
Dopa-Mind™
60 vegetarian tablets Item Catalog Number: 02006
Dopamine is a neurotransmitter that regulates mood and cognition. But dopamine levels decline as we age, corresponding to a decrease in mental performance. Dopa-Mind™ is a unique formula that helps promote healthy dopamine levels to help support and maintain youthful cognitive health.
Benefits at a Glance
Supports mental acuity
Provides longevity benefits
Enhances brain dopamine levels
Contains a potent, standardized extract of wild green oats
MAO-B enzyme and healthy dopamine levels
Dopa-Mind™ contains a standardized extract of wild green oats which inhibits the monoamine oxidase-B (MAO-B) enzyme. This is important, because age-related decline in dopamine is largely caused by rising levels of MAO-B.
Studies indicate promising cognitive health support
Published studies show that by inhibiting MAO-B, this bioactive wild green oat extract promotes healthy dopamine levels. This MAO-B inhibiting mechanism has been shown to support mental acuity and longevity.1
In a double-blind, randomized, placebo-controlled trial in aging volunteers with below-average cognition, researchers demonstrated that 1,600 mg of the same wild green oat extract found in Dopa-Mind™ produced a 74% improvement on a standard test of mental acuity.1
In soon-to-be published research, 800 mg of the same extract supported mental processing time and speed.2 In other research, this extract exhibited support for cerebral vasodilator function, as well as endothelial function — both of which play roles in brain health.3
Breakthrough supplement for memory, cognition, and more
The wild green oat extract in Dopa-Mind™ has been shown to promote more youthful cognitive performance in those where it is showing signs of waning, help maintain cognitive function in those whose minds are still healthy, and may support longevity.
The suggested dose is one tablet of Dopa-Mind™ daily for the first month. If desired results do not manifest, increase the dose to two tablets daily.
Help promote and maintain youthful cognitive performance and longevity. Try Dopa-Mind™ today!
I have taken it for approx 10 years, starting at 1.25mg twice a week, and currently same dose but daily (mornings – sublingual). One thing I have noticed is of course more energy and motivation, but also increased learning abilities similar and sometimes better that what I enjoyed in my twenties. I’m currently mid 60’s, I have taught myself guitar and my hands are loose and able to play quickly,correctly and for long periods of time.
This was a feat I tried to learn in my 20’s and failed at. I also find myself more alert and my reaction time is much better. I’m able to catch falling objects quite easily and have caught flies, mosquitos and moths with my bare hands, usually using just one hand. Also my hand, eye co-ordination is improved and I can catch thrown objects with my left hand almost as well as my right hand (my dominant hand is my right).
so I think there are some interesting learning and memory aspects to this chemical as well as its longevity potential. Also take melatonin at night to help with sleep, and it is also a suspected longevity agent. Also try to sleep in a very dark room.
Informative and relevant article. appreciate it.
Recently our practice prescribes KLAMIN an extract from Alphanizomenon Flos-Aquae (AFA) as adjunct therapy for neurosis, hypochondria and food addiction minus the significant side effects of synthetic MAO inhibitors.
Do you have any research or experience with this botanical extract?
regards,
I just got my prescription for Selegiline and I hope it will help me. Had so much heartaches for most of my life and have gone thru so many ugly trials , so I find myself on the melancholy side, plus I really want to feel better all around. I’m really hoping to see if it wil help me.
It’s over a year since anyone posted in this thread.A quick pubmed search seems to show not much recent interest in selegiline. Any new experiences or insights?
I have started to take 5mg every other day for longevity effects. The tablets are so tiny that taking less is hard to do. I noticed better concentration(which was good already anyway). Also it works as a powerful libidobooster which I intuitively interpret as pro-longevity.
So have you formed any new opinions since writing the article and subsequently starting to take deprenyl ?
18 years ago when I was in my early 60’s I read about a recommendation to begin Selgin at 50 taking 5 mg in the morning and another 5 mg at noon. I began my day with 10mg and have continued without fail. Several years ago while leaving n airlane I found myself standing next to a gentleman who owned a drug manufacturing company in New Jersey. I asked him what he knew about Selgin. “A lot” was his reply. I told him that I had been taking 10 mg daily for 16 years and he told me that it was the smartest thing I had ever done.
Did you notice any improvement to mood, especially libido? Any other benefits you may have noticed?
Table 5 should be updated with:
Stoll 1997: increase in females only: https://www.sciencedirect.com/science/article/abs/pii/S0197458097000092?via%3Dihub
Knoll 2016 (his last study?): https://www.sciencedirect.com/science/article/abs/pii/S0024320516306257
0.001 mg/kg, 3 X per week: no significant effect on average lifespan (but huge effect on shortest!)
0.1 mg/kg, 3 X per week: +12%
(Pleaste notethat Knoll died in 2018 at age 93)
Semmelweis U (Knoll’s university) 2023: BPAP (a deprenyl derivative) doesn’t improve life-span in calory-restricted and intellectually stimulated rats: https://link.springer.com/article/10.1007/s11357-023-00821-6