
Recent re-analysis suggests that Alzheimer’s Disease ought to be ranked with cancer and heart disease as one of the most important mortality risks for older Americans. Some of this risk is under our control.
In a study published last week, Bryan James and colleagues at Rush Univ. Medical Center in Chicago tell us that Alzheimer’s Disease has been greatly under-reported as a cause of death. According to current statistics, cancer and heart disease are tied for the top spot, each contributing almost ¼ of all deaths in the US. The new study says that AD should be right up there with heart disease and cancer, accounting for about ⅕ of US deaths. If they are right, then these Big 3 diseases of old age together account for 70% of all deaths – not just deaths among the elderly.
Previously, AD had been listed as number 6 by the US Center for Disease Control, and the new study would move AD up to the #3 spot, which had previously been claimed by emphysema. Emphysema is way behind cancer and heart disease, and predominantly affects smokers. It’s almost certainly true that AD has been under-reported, and it wouldn’t take very much to move it up to #3; but whether AD really accounts for a 20% risk factor overall is less clear. Let’s take a look at their methodology. (or if you like you can skip ahead: What can you do about your AD risk?)
What’s wrong with this study?
The methodology of the study was straightforward. For eight years, they tracked a group of about 2500 seniors, average age 78. They learned if each person was diagnosed with AD, and if he died. People diagnosed with AD had on average less than 4 years to live. The mortality rate for people diagnosed with AD under age 85 was 4.3 times higher than otherwise (and 2.8 times higher if over 85). These numbers (4.3 or 2.8) are called “hazzard ratios”, and as it turns out, they are an easy statistic to work with, and translate straightforwardly into inferences about the mortality risk of a diagnosis of AD.
The authors make the leap that this many deaths were attributable to AD, whether AD was listed as the cause of death or not. Is this justified? Think about it. They are assuming that AD is the underlying cause and (for example) heart disease might be listed as the cause of death, but the heart disease was caused by an earlier diagnosis of AD. But isn’t it just as likely to be the other way around? People in danger of a heart attack may undergo bypass surgery, as a result of which the brain is deprived of oxygen during surgery and cognitive impairment results.
Or maybe there are underlying conditions (e.g., high inflammation, metabolic syndrome) that put the patient at higher risk for both AD and cancer, and then the patient dies of cancer. It’s not right to assume that AD caused the cancer, or that this patient really died of AD.
So the authors’ conclusion that AD causes half a million deaths in the US every year is certainly overstated. Nevertheless, they’ve got a point, and AD almost certainly should be moved up to the #3 slot, especially for non-smokers. I believe there’s a lot of truth in the idea that mortality from AD is under-reported because the proximate cause of death is frequently something else. If nothing else, depression and institutionalization frequently follow from dementia, and both are major mortality risk factors, under many guises. Also, I believe in an “aging clock”: regulation of the rate of aging that derives from hormones secreted in the brain. It is not hard for me to believe that deterioration of the brain has a direct effect on aging, and through aging on other aspects of health.
Blood test predicts AD
Also reported this week was a blood test that can predict (10 false positives out of 100) who will develop AD in the ensuing three years. The work was reported in Nature Medicine by Howard Federoff of Georgetown University. Does the test offer a clue about the etiology of AD? Not at all. The test was developed using formal statistical methods. They made lipid blood profiles for several hundred people over the age of 70, testing the specific types of fats present in the blood plasma. Then they waited three years to see which of the people might be diagnosed with AD. Then, after the fact, they went back and used a blind, brute-force computer search to test millions of combinations of different features in the lipid profiles to look for ways in which the people who developed AD might be consistently different from the people who didn’t. They then tested the test, applying it to a completely different group of people to see if the same test would work to predict AD for them. It did.
There is no biology in this approach; only mathematics, and authors of the paper do not try to parse the significance of their results.
What causes AD?
Medical science is not in agreement about the cause of AD, and it may be that the symptoms of cognitive impairment come from several causes, separately and together. Up until a few years ago, there was a theory about amyloid plaques in the brain, tiny accumulations of misfolded proteins that the body has failed to recycle. But that theory has faded in popularity with evidence that the plaques may be an effect rather than cause of AD.
Apoptosis of otherwise healthy neurons? or is it
Amyloid plaques triggering an inflammatory attack on the brain?
Everyone agrees that the proximate cause of dementia symptoms is the loss of nerve cells in the brain. Curiously, it seems that healthy neurons may be “committing suicide”, eliminating themselves via apoptosis [ Ref1 , Ref2 , Ref3 ]. For people of my school, this is yet one more instance of the body’s suicide program, the finite life span that has been programmed into our genes by natural selection for the purpose of leveling the death rate and stabilizing ecosystems. People who believe that aging is not programmed tell the story in terms of the amyloid plaques triggering an immune response, and it is the inflammation that leads to apoptosis. In any case, we all agree that inflammation is a risk factor for AD, and that anti-inflammatory supplements and drugs can lower the risk of AD. (Anti-inflammatories also offer protection against cancer and heart disease.)
What can you do control your risk of AD?
The usual stuff. Weight control, exercise, and most everything else you do to extend life expectancy lowers risk of AD along the way. Remaining mentally active, learning new skills, putting yourself in new situations and taking on new challenges – these are ways to keep ourselves alive and aware, and they also reduce risk of AD
Anti-inflammatories are especially helpful. Curcumin (turmeric) is an herbal anti-inflammatory that deserves special mention because of the many studies finding a protective effect in test tubes, mice, and humans. In India, dementia is only ¼ as common as in Europe and America, possibly because of turmeric in the diet. There is evidence to recommend fish oil, and also studies in which fish oil does not work. Daily, low-dose ibuprofen lowers the risk of AD, and there are mixed reports of whether aspirin does as well.
A great number of traditional herbs have been shown to be neuroprotective. This review of neuroprotective herbs mentions Ashwaghanda, Bacopa, Carnitine, Melatonin, CoQ10, Garlic, Vitamin D, Ginseng, and Ginkgo biloba. Here is another review of herbs that might be useful for AD. None of these is a cure for AD, but there is some clinical evidence for benefit from each. Readers familiar with my AgingAdvice page know that I like melatonin and vitamin D for other reasons as well.
Blueberries and perhaps other berries are protective. A substance called fisetin (chemical cousin of quercetin) found in fruits and berries may be partly responsible. Soy products contain phytoestrogens – chemicals which resemble female hormones. Twenty years back, it was noticed that east Asians who moved to America and adopted an American diet had lower risk of AD, and it was hypothesized that phytoestrogens from soy might increase risk of AD. But more recently several studies seem to point in the opposite direction, that soy might protect against AD [ Ref1 , Ref2 , Ref3 ].
I’ve reported (here and here) that since November I’ve been taking deprenyl (~1mg daily) and I find that it’s making me happy and increasing my energy, much to my consternation since I’m constitutionally anti-anti-depressant. Deprenyl (sold as Selegiline or Emsam) is neuroprotective and it’s on the short list of drugs that consistently augment the life span of rodents in the lab.
And what is the payoff for avoiding AD?
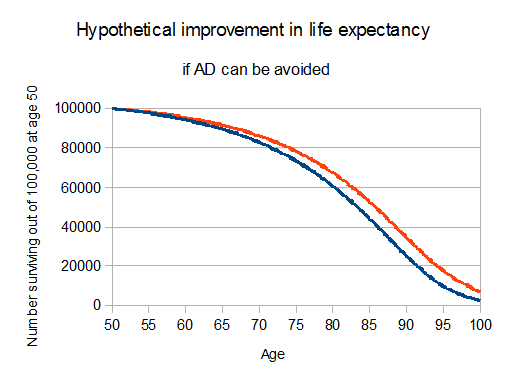
According to the new hypothesis of James, 20% of mortality risk at all ages comes directly or indirectly from dementia. Based on a 20% reduction in mortality, I calculate (using CDC life tables for 2010) that if we can greatly reduce risk of AD with all the above measures, starting (for example) at age 50, we might add 2½ years to life expectancy.
A horrible way to die, for some
The stereotypical AD patient is depressed and isolated by failure of his memory and inability to communicate. And sadly, this is the norm as patients become disoriented and frustrated with inability to function. But some AD patients become happy and grateful, detached from the worries that tied them down, occasionally euphoric.
Who will I be after I die? Who was I before I was born?
We think of life and death like 1 and 0, like on and off, without a gray zone. But it took time for our physical selves to develop, and our brains to connect up in ways that support the conception of a separate self. In AD, the self takes about the same amount of time to disintegrate as it took to form.
Most of us have no memories before we were three. Perhaps it takes three years for the brain to organize itself around time and events, inner self and outer world. All that individuation that happened during the “terrible twos” is no longer part of our remembered life. All that bewilderment, the wonder and constant questioning, a state of deep becoming.
I think of AD as the mirror image of the child’s individuation, the gradual dissolution of self. For many of us, that prospect is terrifying, but remember that the infant also found it terrifying to become a separate self. If there’s any benefit we can hope to derive from a lifetime of accumulated wisdom, let it be the ability to know fear for what it is: merely a genetic program, evolved to protect the individual genome and improve our chances of passing
When you say “daily, low-dose ibuprofen” what dosage do you mean? 200 mg? Is it likely better to take is with food or on an empty stomach?
200 mg or less. There is no data to support more as better. But there may be other reasons to take a little more. For example, I find I am more flexible in yoga and less stiff after running if I take a full ibuprofen or aspirin.
The empty stomach question is about your comfort. Some people get upset stomachs if they take aspirin or ibuprofen without food. You know if you’re one of them.
What do you think of this paper?
https://www.nature.com/articles/437045a
This would be another supporting evidence for the Mediterranean diet.
50 g/day of newly pressed extra-virgin olive oil may be a safer bet than low-dose aspirin or ibuprofen.
The problem is with the “newly pressed” qualifier.
I wonder if freezing the extra-virgin olive oil can maintain the oleocanthal.
Hi Josh,
One element of this topic that seems interesting is related to your idea with which I agree, that aging is a result of a clock mechanism in the brain that mediates aging via hormones. When you consider the full spectrum of brain diseases, cell death can occur in any part of the brain and at any stage of life which will result in reductions in any kind of known or unknown brain produced hormones by loss of cells that produce such hormones. Since we do not have examples in nature where people or animals with or without significant brain disease do not senesce, it is apparent that the any such aging clock is likely functioning as the result of a reduction in one or more hormones. This logic argues for the conclusion that one or more hormones sustain the non-senescent state and reductions in one or more of these substances results in the production of the senescent phenotype.
A few hormones (peptides) that I think could be candidates for senescence regulation could be , Growth Hormone Releasing Hormone (somatotropin), and its counterpart Growth Hormone Releasing-Inhibiting Hormone ( Somatostatin).
Kevin Brown
Yes – and it also may be more complicated than this, because there are definitely hormones we have too much of as we age, LH and FSH for example. http://joshmitteldorf.scienceblog.com/2013/11/12/molecules-in-the-blood-that-signal-self-destruction/
Yes, LH and FSH appear to be players in overt death mechanisms. They are highly conserved in evolution as they also function in fish in a similar way. But I think the question is, are they at the top of the hierarchy of control as part of the clocking mechanism of aging? At least, I think we can say that considering that both fruit fly experiments by M. Rose and field studies on opossums sequestered on islands have demonstrated that evolution seems highly capable of manipulating the rate of senescence in a species very quickly in generational time. This supports the idea that there must be very few factors at the actual top of the hierarchy commanding the processes of senescences. If senescence was mediated by a network of autonomously acting agents it seems far less likely that rates of senescence could be manipulated so easily.
I have to share a private experience of irony. I had dinner with Aubrey de Grey last night, and he made exactly the opposite argument: He said that if aging were programmed, then it would respond much more rapidly to selection pressure than in the Austad experiment. I don’t understand why either fast or slow response should be our expectation, and how this depends on the hypothesis of programmed aging.
Josh,
Nice article. However, in regard to AD etiology, you did not mention the work of the neurologist J. Miklossy which finds that 90% of autopsied AD brains that were studied are infected with pathogenic spirochetes. It turns out that the Lyme bacterium is spirochetal, and it constitutes 25% to the 90% figure above. The remaining 65% are spirochetes that originate in the oral cavity and make their way to the brain via the bloodstream or via nerve pathways that run between the brain and the mouth.
Please note that syphilis is caused by a spirochetal bacterium, and that disease is known to be capable of causing dementia. Therefore, it is highly likely that spirochetal infection is the cause of AD. The entire article is available for free at: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3171359/
If you would like a quick synopsis of the article before looking at it yourself, the following may be helpful:
1. Lyme disease and syphilis are both caused by spirochetal bacteria.
2. Syphilis is known to cause dementia. Maybe Lyme (and other spirochetes) do too.
3. Lyme bacteria are found in 25% (this is 13 times higher than in the control population) of autopsied Alzheimer’s brains. An additional 65% of such brains are found to be infected by other pathogenic spirochetes which originate in the mouth. These percentages are statistically significantly higher than in the general population.
4. The bacterial infection described above is co-located with the Alzheimer’s plaques.
5. The A-Beta protein which accumulates in Alzheimer’s brains is an anti-microbial protein. This suggests that its proliferation may be a physiological response to infection.
6. When mammalian neural cells are cultured with added Lyme bacteria in a petri dish, the characteristic pathological hallmarks of Alzheimer’s disease (i.e plaque build-up, etc.) are found to occur.
Finally, the best book we have right now on how to treat spirochetal infection in humans is by Richard I Horowitz, MD and has the title: “Why can’t I get Well: Solving the Mystery of Lyme and Chronic Disease”.
Best wishes,
Peter Kraus